![]()
Presentation
American Association of Clinical Endocrinologists Scientific & Clinical Congress
Date
May 2013
Authors
Joseph Aloi,1 Raymie McFarland,2 Margaret Bachand,3 Courtenay Harrison3
Objective
Ongoing efforts at improving quality metrics in the care of persons with diabetes frequently focus on avoiding unnecessary hospitalizations, decreasing length of stay and avoiding readmission to hospital following discharge. Our prior experience with Glucommander, a web based insulin dosing algorithm, in inpatient insulin protocols suggested that its use in the emergency department (ED) would be safe. We previously studied the effectiveness of the Glucommander system for the treatment of mild to moderate Diabetic Ketoacidosis (DKA) in the ED and reported early data on 15 patients. We now report a full 1 year experience with 35 patients studied.
DKA is a frequent cause for hospital admissions – accounting for up to 8% of general medicine admissions in some hospital studies.4 Current standard treatment protocols involves use of intravenous insulin infusions monitored in the intensive care unit (ICU); raising both the cost and complexity of care.
Methods
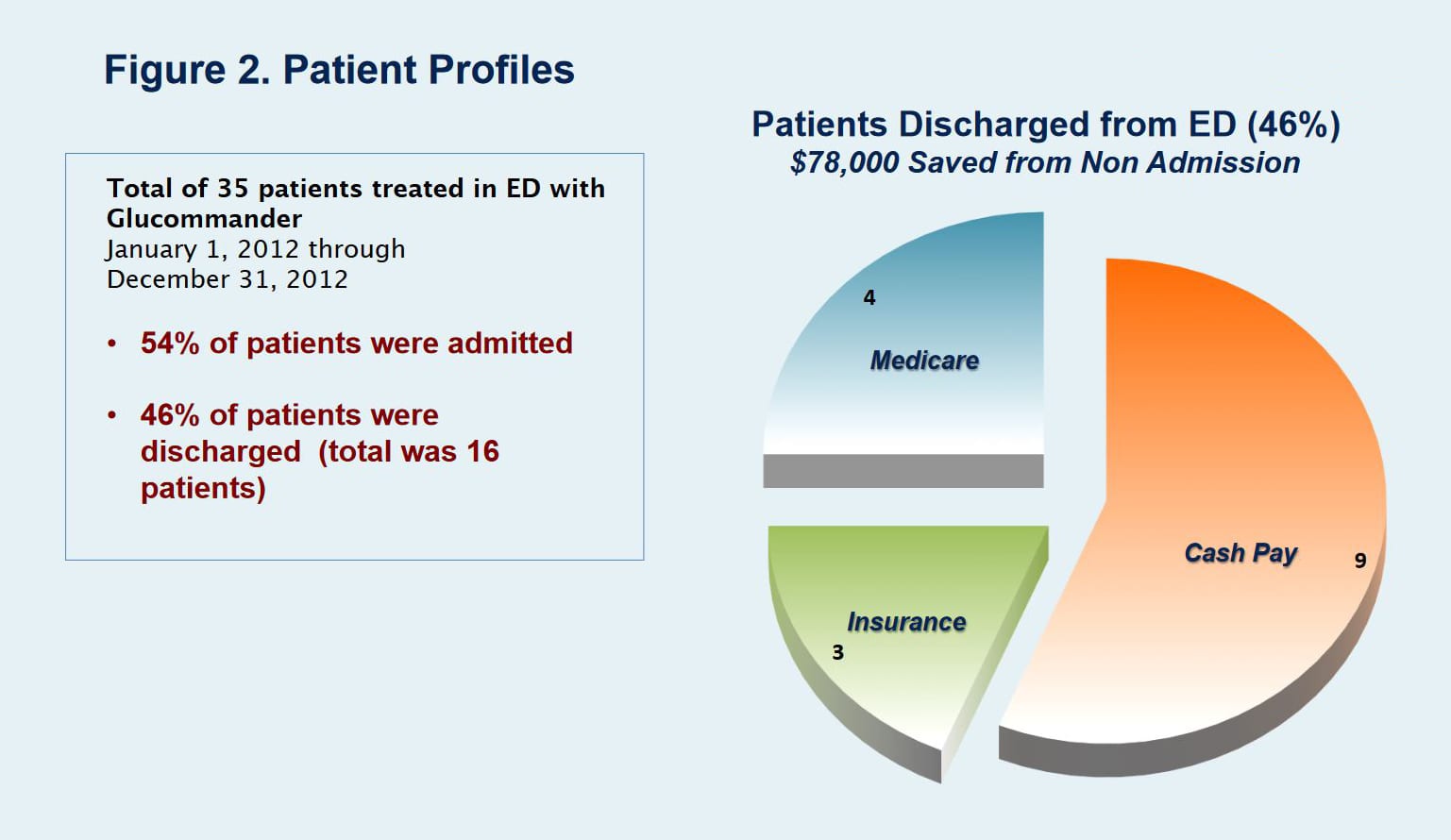
35 Patients seen in the ED diagnosed with DKA during the 2012 calendar year were reviewed. All patients were studied at a single site – Virginia Beach General Hospital (VGBH) a 300 bed community hospital within the Sentara healthcare system. Patients seen in the ED with either significant hyperglycemia (glucose >300 mg/dL) or DKA were placed on the Glucommander protocol. Patients were then monitored for readiness to be discharged or need for admission.
Adult patients with blood glucose >250 mg/dL, a positive anion gap and/or ketonuria were eligible to participate. Patients with severe acidosis (pH <7.0 or serum bicarbonate <10 nmol/L), or a concomitant medical illness requiring hospitalization (e.g. pneumonia or congestive heart failure) were excluded from the protocol.
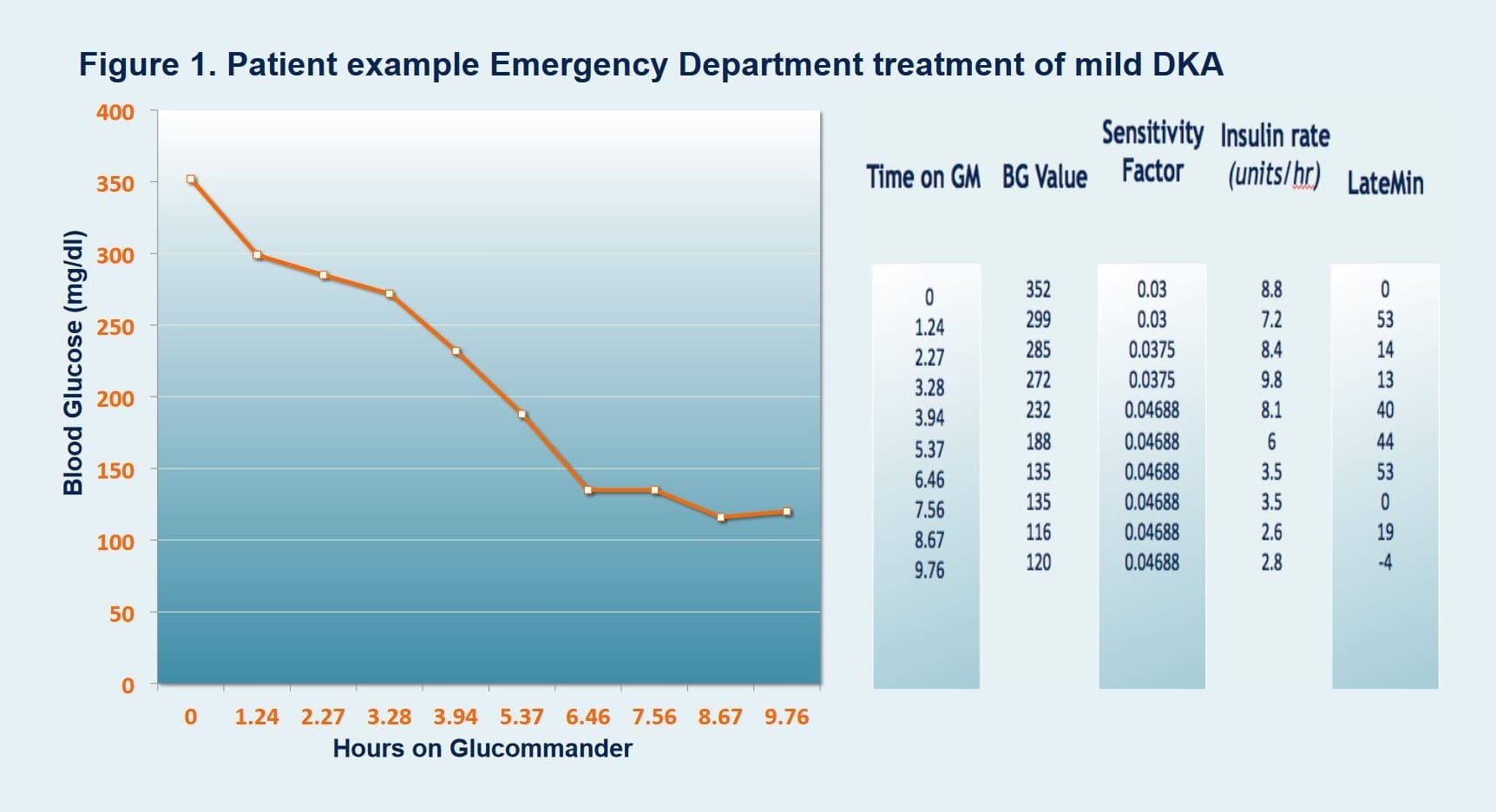
The Glucommander used the variables of patients’ height, weight, and current and cumulative BG values to determine the algorithm-driven recommended dose of insulin or glucose to reduce individual patient BG levels into a predetermined glycemic range.
Results
The web based algorithm, was able to manage hyperglycemia effectively. Initial average blood glucose (aBG) on presentation = 487 mg/dL, time to target BG = 4 hours 41 minutes, aBG = 145 mg/dL +/- 34; with low rates of Hypoglycemia (BG <70) rate of less than 0.4 %. Approximately 50% of patients treated with the protocol were able to be discharged from the ED directly or in one instance held for short stay observation. We found no evidence of readmission to the Sentara Healthcare system within 30 days of discharge from the ED for DKA for the study group. Nursing satisfaction scores remained high using the tool for DKA. No significant adverse events were noted.
IV Insulin Therapy in the Intensive Care Unit Over a 12 Month Period
| Total Patients | 35 |
|---|---|
| Average Initial BG | 487 mg/dl |
| Average BG | 145 mg/dl +/- 34 |
| Average Time to Target | 5 hours 11 minutes |
| Average Time on G+™ | 14 Hours |
| Hypoglycemia <70 mg/dl | 0.3% (18 BGs) |
| Hypoglycemia <40 mg/dl | 0.0% (0 BGs) |
| Hyperglycemia >250 mg/dl post D50 | 0.0% (0 BGs) |
| Total Number BGs | 490 |
| Patients Admitted to Hospital from ED | 54% |
| Patients Discharged Home from Hospital ED | 46% |
Conclusion
Use of a web based insulin infusion algorithm in the ED can decrease admissions to hospital for DKA by almost 50%. Ease of use coupled with low rates of hypoglycemia makes this an attractive option to improve efficiency of utilization of inpatient hospital beds. The cost savings for non-admissions was estimated at $78,000 over the 12 months of the study. Our results suggest that Glucommander is a safe and efficient tool for use in the ED to manage mild to moderate DKA.
Affiliations/References
- Virginia Medical School, Division of Endocrinology and Metabolism Eastern, Norfolk, Virginia.
- Glytec, Quality Initiatives Division, Greenville, South Carolina.
- Virginia Beach General Hospital, Sentara Healthcare, Virginia Beach, Virginia.
- Subcutaneous lispro and IV regular insulin treatments are equally effective and safe for the treatment of mild and moderate DKA in adult patients; Ersoz et al. The International Journal of Clinical Practice Mar 2006.