![]()
Publication
Journal of Diabetes Science and Technology
Date
December 2014
Authors
Christopher Mulla,1 David Lieb,2 Raymie McFarland,3 Joseph Aloi2
Introduction
This study explores the relationship between education for inpatient diabetes providers and the utilization of insulin order sets, inpatient glucometrics, and length of stay in a large health care system. The study included patients with and without the diagnosis of diabetes. An education campaign included provider-directed diabetes education administered via online learning modules and in-person presentations by trained individuals. Relationships among provider-attended diabetes education, order set usage, and inpatient glucometrics (hypo- and hyperglycemia) were analyzed, as well as length of stay. Insulin use knowledge scores for all providers averaged 52%, and improved significantly to 93% (P < .001) by the end of the education intervention period. Likewise utilization of electronic basal-bolus order sets increased from a baseline of 20% for patients receiving insulin to 86% within 6 weeks (P < .01) of introduction of order sets. During the study, the incidence of hypoglycemia and hyperglycemia declined from 1.47% to 1.27% and from 23.21% to 17.80%, respectively. However, these improvements were not sustained beyond the completion of the education campaign. Education of diabetes health care providers was provided in a large, multihospital system through the use of online learning modules. Adoption of standardized insulin order sets was associated with an improvement in glucometrics. This educational and quality initiative resulted in overall improvements in insulin knowledge, adherence to recommended order sets, inpatient glucometrics, and patient length of stay. These improvements were not sustained, reinforcing the need for repeated educational interventions for those involved in providing inpatient diabetes care.
Improving inpatient glycemic control is an area of focused quality improvement in United States hospital systems, and was recently championed by the consortium for Planning Research in Inpatient Diabetes. Inpatient hyperglycemia is common and affects up to 40% of all hospitalized patients, and may be present in up to 70% of those patients presenting with an acute coronary syndrome.1 Hyperglycemia is also associated with significant adverse outcomes, including increased mortality and increased length of hospitalization.2,3 Many inpatients require insulin to control their glucose, a medication that carries a significant risk of hypoglycemia and its associated morbidity.4,5 Though data from observational studies suggest that hyperglycemia is detrimental for hospitalized patients, the optimum glucose range in these patients is less clear. Randomized controlled trials in the intensive care setting have suggested both benefits and harms associated with tight glucose control, and outcomes appear to differ between medical and surgical patients.6-8 Less data are available with regard to patients in the non-critical-care setting. In 2009 the American Association of Clinical Endocrinologists and the American Diabetes Association published a consensus statement regarding inpatient glucose control.9 The authors recommended a number of research questions for future studies to address, including what hospital systems are necessary to improve both inpatient glucose control as well as patient safety.9
Inpatient glucose control involving an inpatient diabetes team, provider and staff education, and well-developed protocols has been associated with both improved costs and decreased length of stay.10,11 Education, in particular, is a critical part of developing an inpatient glycemic program. Insulin preparation, prescription, and administration involve multiple providers, including pharmacists, physicians, and nurses. Dedicated educational programs for nurses, medical trainees, nurse practitioners, physician assistants, and physicians have resulted in improvements in inpatient glucometrics, defined as the analysis and reporting of significant hypoglycemic and hyperglycemic events in a hospital setting.12-15 The introduction of electronic medical record platform-based insulin order entry with standardized insulin order sets has improved the proper use of insulin in the hospital.16 However, the implementation of such changes can be complex when involving large hospitals and multisite hospital systems.
This article describes a quality improvement project conducted in an integrated multihospital health care system in southeastern Virginia (including Sentara Healthcare and Eastern Virginia Medical School). The aim of this quality improvement project was to determine if an education campaign coordinated with implementation of electronic insulin order sets would increase adherence to practice guidelines in insulin usage, and improve glucometrics and patient outcomes in a large multihospital system. We describe the journey and experience of our own organization and demonstrate the importance of measuring and understanding glucometrics in the hospitalized patient population. Our study reinforces not only the importance of integrating technology in improving inpatient glucometrics across a large number of patients but also the need for repeat education and assurance that providers understand the significance of adopting new technology.
Methods
Setting, Practitioners, and Patients
This quality improvement project was reviewed by the Eastern Virginia Medical School Institutional Review Board. All data collected were in aggregate form and not linked to an individual’s personal health information. The project was conducted in an integrated health care system in southeastern Virginia that includes 7 hospitals and a total of 1760 patient-beds. Approximately 22000 patients who were hospitalized and available for review annually between 2008 and 2011 were analyzed in this project, including those with a discharge diagnosis of diabetes that were retrospectively identified. Following the adoption of an electronic medical record (EMR), the EMR was used to enter all insulin orders (Epic; Epic Systems Corporation, Verona, WI). An educational campaign was designed and conducted over a 3-month period between November 2009 and January 2010. Inpatient blood glucose and length of stay data were reviewed for the years 2010 through 2012. Critically ill and non-critically ill patients were included, as well as all general medical and surgical patients. Various health care professionals were involved in ordering and adjusting insulin in this study, including physicians, physicians in training, and midlevel providers. A concerted educational campaign specifically directed to appropriate insulin usage and managing inpatient hyperglycemia was offered to all licensed providers, nurses, residents, and pharmacists. This took the form of computer-based learning modules, didactics, and lectures.
Glycemic Control Committee
A glycemic control committee was developed to create appropriate educational materials and to assist with the implementation and use of electronic insulin order sets. The committee included representative endocrinologists, nursing administrators, pharmacists, hospital administrators, and internal medicine residents and met regularly for 3 months prior to starting the project. The committee developed orders sets incorporating the use of basal-bolus insulin (BBI) regimens, and eliminated the use of more traditional sliding-scale insulin (SSI). They also encouraged the use of more rapid-acting analogue insulin rather than regular insulin. Rapid-acting analogs were chosen as they have been associated with improved inpatient glycemic control and allow nurses to give insulin with meals in patients with unpredictable diets.17,18 The glycemic control committee identified “champions” that included physicians, pharmacists, nurses, and case managers, who were selected to develop and deliver study-related education.
Study Intervention
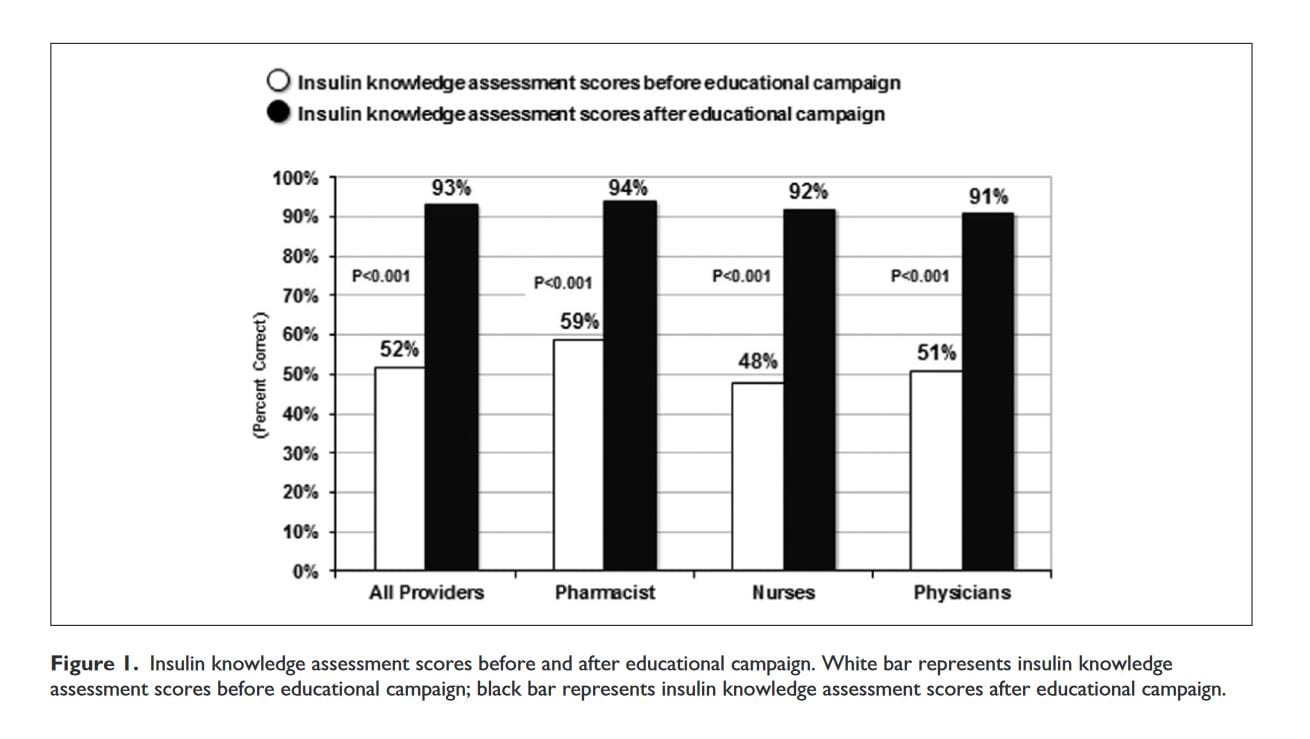
Education Campaign. The education campaign included both online webinars and live in-person lectures. Providers were given insulin-prescribing guidelines on a laminated card for easy use. Knowledge assessment regarding inpatient glycemic management with insulin was completed before and 4 weeks after the education campaign by nurses, pharmacists, and physicians. The knowledge assessment tool included 25 questions and was based on the Johns Hopkins Insulin Knowledge Tool.19
Order Set Implementation. Several interventions were implemented to discourage the use of SSI, to support BBI orders, and to reduce the use of regular insulin. Paper SSI order sheets were completely removed. When an EMR was utilized, attempts to enter SSI orders brought up a warning message indicating that best practices would recommend the use of the new BBI order set.
Glucose and Hospital Patient Metrics. Both point-of-care finger-stick blood glucose samples and plasma glucose samples were included in the determination of average blood glucose during each patient’s hospitalization. When determining effects of the education campaign and order set changes on length of stay, patients were divided into 4 groups: nondiabetic patients, diabetics admitted for a diabetes-related condition, diabetics admitted for a non-diabetes-related condition, and patients without a known history of diabetes who developed hyperglycemia following admission for a non-diabetes-related problem.
Statistics
Statistical analysis was performed by Atlanta Diabetes Associates. Chi-squared tests were used for all the analysis as follows: hypoglycemia (percentage blood tests < 70 mg/dL) and hyperglycemia (percentage blood tests > 180 mg/ dL) were compared in each interval time in the consecutive data series as compared to baseline. The utilization of BBI orders was determined as the percentage of patients prescribed compared between each data set and the next consecutive data set in the timeline. Education test scores were analyzed as the percentage correct answers compared between the preeducation period and the posteducation period. This was done for 3 different job descriptions and for the combined set of job descriptions.
Results
Prior to initiation of the education campaign, 344 nurses, 138 pharmacists, and 85 physicians were given the insulin knowledge assessment tool (Figure 1). The average preeducation campaign score among all providers was 52% correct. Four weeks after the education campaign the insulin knowledge assessment tool improved significantly to an average of 93% (P < .001) correct. There were no significant differences between the different providers before or after the campaign.
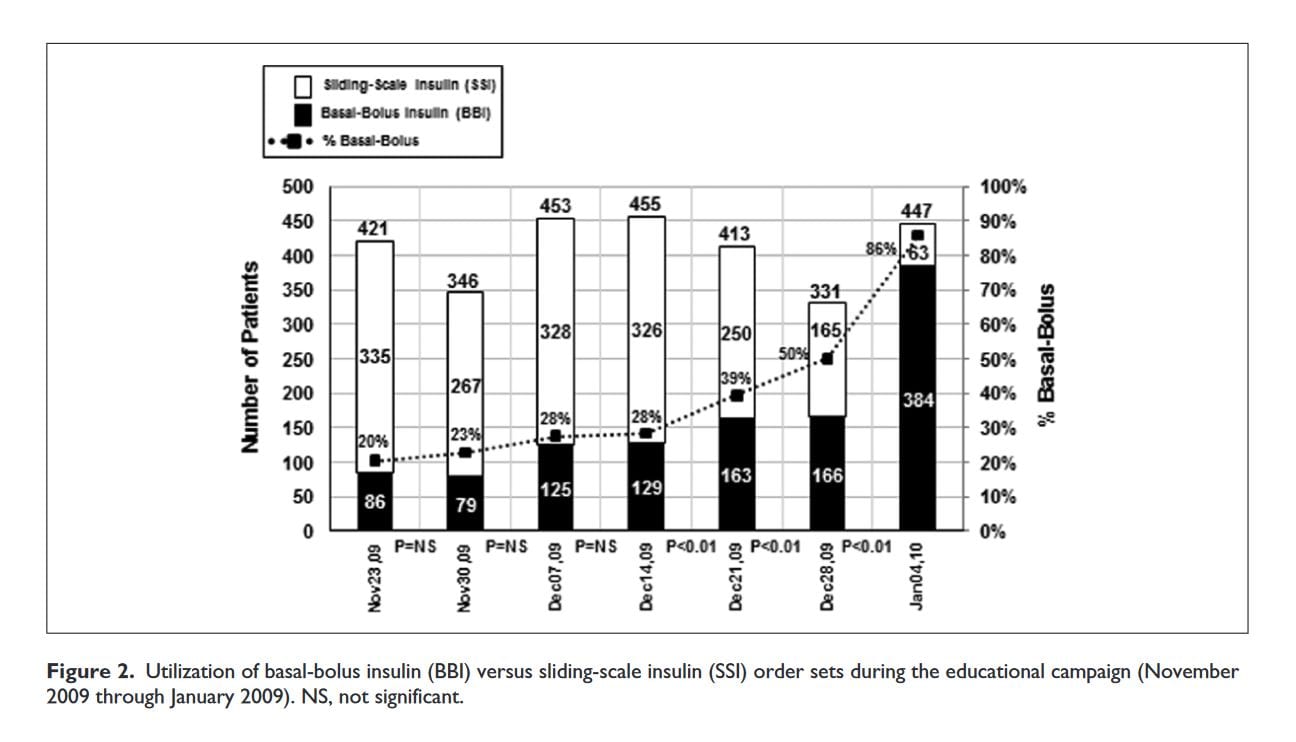
The utilization of BBI order sets increased significantly during the education campaign (Figure 2). Prior to the start of the education campaign, only 20% of the insulin orders were basal-bolus orders. By the end of the education campaign period this had increased to 86% (P < .01). The utilization of basal-bolus orders remained > 90% for the remainder of the study period (data not shown).
The changes in insulin orders corresponded to improvements in average glucose readings. Prior to the initiation of the education campaign, the percentage of finger-stick hypoglycemic events (defined as a glucose < 70 mg/dL) was 1.47% but improved following the education period to 1.24% (P = NS) (Figure 3).
Subsequently, the hypoglycemia rates increased in 2010 to 2.66% (P < .001), but then began falling (to 2.17%) by 2012. During the period 2009-2010 there was a reduction in the percentages of hyperglycemic events (defined as a glucose > 180 mg/dL) from 23.21% of inpatient glucose readings to 17.80% (P < .001) at the end of the education campaign (Figure 4).
Incidence of hyperglycemia followed a similar trend as hypoglycemia after the intervention, initially increasing in 2010, then making gradual improvements each year.
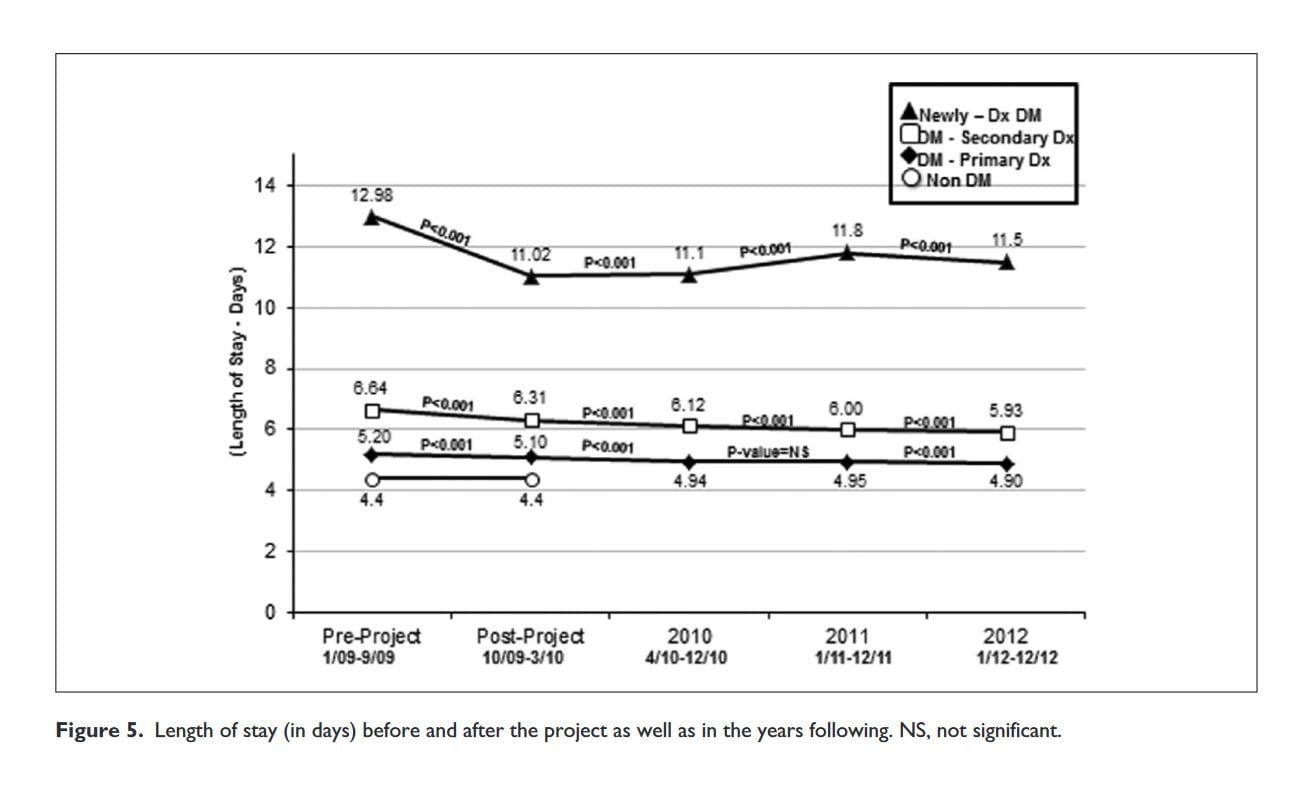
Changes were observed in the length of hospital stay after our intervention in patients with diabetes from 6.64 to 6.31 (P < .001), and especially in those hyperglycemic patients who did not have a previous diagnosis of diabetes 12.98 to 11.02 (P < .001) (Figure 5).
The average length of stay in the hospital for nondiabetic patients did not change during the study period 4.4 to 4.4, highlighting the effect of intervention on the length of stay reduction for the different hyperglycemic groups.
Discussion
This study describes a large, multihospital intervention involving both an online educational component and the use of insulin orders sets incorporated into an EMR. We developed an educational campaign partnered with an inpatient basal-bolus electronic order set followed by the implementation of that project into 7 large hospitals servicing over 20 000 patients annually. We show improvements in medical knowledge across a variety of providers and significant adherence to the new protocols. We noted significant improvements in our glucometrics, including a significant reduction in hyperglycemia, and a nonsignificant reduction in hypoglycemia. These improvements were coupled with reductions in length of stay for our diabetic patients. In particular, we noted almost a 2-day reduction in length of stay in diabetic patients who had not been diagnosed with diabetes prior to admission. This reduction in hospital stay could result in over 1300 fewer hospital days and a savings over $2 million yearly. The length of stay remained unchanged for the remainder of the period observed—though glycemic rates regressed to baseline values. This suggests that the length of stay improvement may be more related to standard insulin order sets than specific glucometrics. Interestingly we saw increases in both hypo- and hyperglycemia after the completion of the project, reinforcing the importance of and need for continued education.
Of note, our intervention coincided with a transition from paper charts to an EMR across the organization, with full transition completed in all of the hospitals by September 2010. Two of the 7 hospitals had not transitioned to an electronic order set at the time that study data were collected, though all order sets were available in all hospitals (either paper or electronic).
Health care providers’ lack of knowledge with regard to appropriate insulin use is an under appreciated obstacle to successful achievement of glycemic goals in the inpatient setting. Derr et al collected almost 400 insulin knowledge surveys from nurses, residents, general medicine attending’s, and subspecialists in their hospitals.19 They demonstrated that overall insulin knowledge scores were < 60% correct. We assessed baseline knowledge of insulin use in a diverse group of health care providers and found that the percentage of questions answered correctly was approximately 50%, consistent with those previously described.19 Following our education campaign, respondents demonstrated a significantly improved understanding of appropriate insulin use in the hospitalized patient. This has been demonstrated in previous studies including residents, nurses, and midlevel providers.13,16
McIver et al published their experience implementing new insulin order sets over 4 hospitals in Queensland, Australia.20 BBI orders have been demonstrated to lead to less stacking of insulin doses, resulting in fewer sustained hyperglycemic and fewer hypoglycemic events, and are the advocated regimen for insulin-requiring diabetics by various medical organizations.9,21,22
In our project we were able to see improvements in hospital glucometrics (both hyperglycemia and hypoglycemia) after implementing new electronic BBI order sets in our health care organization. The result was not sustained following completion of the campaign, with slow rises in both hypo- and hyperglycemia. Several explanations for improvements not being sustained exist including the changing nursing and resident staff seen at the hospitals. Nursing and resident staff turnover would dilute the benefit of a time-limited educational campaign. Hospital staff turnover has been shown to decrease adherence to policy and increase adverse outcomes such as medication errors.23 One systematic review of studies describing the effects of trainee turnover on patient outcomes demonstrated that there was an increase in rate of errors, decreased efficiency, and increased mortality during the July transition of new house staff to hospitals. 24Intermittent educational campaigns may be adequate to improve outcomes as the knowledge obtained may be durable. Another possible reason for the slippage of the achieved results could be following orders with daily titration through basal bolus order sets. Chart reviews post project revealed a trend toward ordering basal bolus but not systematically titrating to glycemic goals.
Similar to our findings, Newton and Young reported that implementation of a new diabetes program in their hospital reduced the length of stay for diabetic patients leading to over $2 million in savings in 1 year.25 We also noted a reduced length of stay for patients who were diagnosed with diabetes during their hospitalization. This reduced hospital stay could be due to increased awareness and more rapid achievement of euglycemia with a regimen that could be continued after the patient was discharged.
A shortcoming of this observational study is that not all of the hospitals’ physicians participated in the educational campaign, yet patients for whom they cared were included in the study results.
Conclusion
The current study demonstrates that a targeted educational campaign along with the introduction of BBI order sets and an EMR-based ordering system leads to improvements in glucometrics across a multihospital system as well as insulin knowledge in providers and staff. The targeted educational campaign led to a 41% (P < .001) improvement in insulin knowledge test scores. The quality improvement project coupled with a transition to EMR-based ordering was associated with a decrease in the incidence of hypoglycemic events from 1.47% to 1.27% (P = NS) as well as a decrease in hyperglycemic events 23.21% to 17.80% (P < .001). Length of stay was reduced by 0.33 to 1.96 days in the hyperglycemic patient groups but remained unchanged in the nonhyperglycemic patient population. These results suggest benefits to the hospitalized patient with hyperglycemia by incorporating standardized insulin order sets coupled with educational programs managed by a glycemic control committee.
Acknowledgments
The authors would like to thank Dr Paul Chidester, MD, VPMA, Sentara Norfolk Hospital, for championing the initiation of the Sentara Glycemic Control Committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Affiliations
- Eastern Virginia Medical School, Department of Medicine, Norfolk, Virginia.
- Eastern Virginia Medical School, Department of Medicine, Strelitz Diabetes Center for Endocrine and Metabolic Disorders, Norfolk, Virginia.
- Glytec Systems, Greenville, South Carolina.
References
- Draznin B, Gilden J, Golden SH, et al. Pathways to quality inpatient management of hyperglycemia and diabetes: a call to action. Diabetes Care. 2013;36(7):1807-1814.
- McDonnell ME, Umpierrez GE. Insulin therapy for the management of hyperglycemia in hospitalized patients. Endocrinol Metab Clin North Am. 2012;41(1):175-201.
- Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of inhospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab. 2002;87(3):978-982.
- Eiland L, Goldner W, Drincic A, Desouza C. Inpatient hypoglycemia: a challenge that must be addressed. Curr Diab Rep. 2014;14(1):445.
- Krinsley JS, Grover A. Severe hypoglycemia in critically ill patients: risk factors and outcomes. Crit Care Med. 2007;35(10):2262-2267.
- van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345(19):1359-1367.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354(5): 449-461.
- NICE-SUGAR Study Investigators, Finfer S, Chittock DR, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283-1297.
- Moghissi ES, Korytkowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care. 2009;32(6):1119-1131.
- Olson L, Muchmore J, Lawrence CB. The benefits of inpatient diabetes care: improving quality of care and the bottom line. Endocr Pract. 2006;12(suppl 3):35-42.
- Levetan CS, Salas JR, Wilets IF, Zumoff B. Impact of endocrine and diabetes team consultation on hospital length of stay for patients with diabetes. Am J Med. 1995;99(1):22-28.
- Ena J, Casañ R, Lozano T, Leach A, Algado JT, Navarro-Diaz FJ. Long-term improvements in insulin prescribing habits and glycaemic control in medical inpatients associated with the introduction of a standardized educational approach. Diabetes Res Clin Pract. 2009;85(2):159-165.
- Herring R, Pengilley C, Hopkins H, et al. Can an interprofessional education tool improve healthcare professional confidence, knowledge and quality of inpatient diabetes care: a pilot study? Diabet Med. 2013;30(7):864-870.
- Vaidya A, Hurwitz S, Yialamas M, Min L, Garg R. Improving the management of diabetes in hospitalized patients: the results of a computer-based house staff training program. Diabetes Technol Ther. 2012;14(7):610-618.
- Yu CHY, Sun XH, Nisenbaum R, Halapy H. Insulin order sets improve glycemic control and processes of care. Am J Med. 2012;125(9):922-928.e4.
- Schnipper JL, Ndumele CD, Liang CL, Pendergrass ML. Effects of a subcutaneous insulin protocol, clinical education, and computerized order set on the quality of inpatient management of hyperglycemia: results of a clinical trial. J Hosp Med. 2009;4(1):16-27.
- Uy J, Fogelfeld L, Guerra Y. Cumulative clinical experience with use of insulin lispro: critical appraisal, role in therapy, and patient considerations. Diabetes Metab Syndr Obes Targets Ther. 2012;5:1-10.
- Guerra YS, Lacuesta EA, Yrastorza R, Miernik J, Shakya N, Fogelfeld L. Insulin injections in relation to meals in the hospital medicine ward: comparison of 2 protocols. Endocr Pract. 2011;17(5):737-746.
- Derr RL, Sivanandy MS, Bronich-Hall L, Rodriguez A. Insulin-related knowledge among health care professionals in internal medicine. Diabetes Spectr. 20(3):177-185.
- McIver FB, Mitchell CA, Finn CP, Kamp MC. Standardizing practices through form design and education improves insulin management. Aust Health Rev. 2009;33(3):434-441.
- American Association of Diabetes Educators. Diabetes inpatient management. Diabetes Educ. 2012;38(1):142-146.
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care. 2007;30(9):2181-2186.
- Bae SH, Mark B, Fried B. Impact of nursing unit turnover on patient outcomes in hospitals. J Nurs Scholarsh. 2010;42(1): 40-49.
- Young JQ, Ranji SR, Wachter RM, Lee CM, Niehaus B, Auerbach AD. “July effect”: impact of the academic year-end changeover on patient outcomes: a systematic review. Ann Intern Med. 2011;155(5):309-315.
- Newton CA, Young S. Financial implications of glycemic control: results of an inpatient diabetes management program. Endocr Pract. 2006;12(suppl 3):43-48.