Randomized Controlled Trial of Intensive Versus Conservative Glucose Control in Patients Undergoing Coronary Artery Bypass Graft Surgery: GLUCO-CABG Trial
![]()
Publication
Diabetes Care
Date
September 2015
Authors
Guillermo Umpierrez,1 Saumeth Cardona,1 Francisco Pasquel,1 Sol Jacobs,1 Limin Peng,2 Michael Unigwe,1 Christopher Newton,1 Dawn Smiley-Byrd,1 Priyathama Vellanki,1 Michael Halkos,3 John Puskas,3 Robert Guyton,3 Vinod Thourani3
ABSTRACT
Objective: The optimal level of glycemic control needed to improve outcomes in cardiac surgery patients remains controversial.
Research Design and Methods: We randomized patients with diabetes (n = 152) and without diabetes (n = 150) with hyperglycemia to an intensive glucose target of 100-140 mg/dL (n = 151) or to a conservative target of 141-180 mg/dL (n = 151) after coronary artery bypass surgery (CABG) surgery. After the intensive care unit (ICU), patients received a single treatment regimen in the hospital and 90 days postdischarge. Primary outcome was differences in a composite of complications, including mortality, wound infection, pneumonia, bacteremia, respiratory failure, acute kidney injury, and major cardiovascular events.
Results: Mean glucose in the ICU was 132 + 14 mg/dL (interquartile range [IQR] 124-139) in the intensive and 154 + 17 mg/dL (IQR 142-164) in the conservative group (P <0.001). There were no significant differences in the composite of complications between intensive and conservative groups (42 vs. 52%, P = 0.08). We observed heterogeneity in treatment effect according to diabetes status, with no differences in complications among patients with diabetes treated with intensive or conservative regimens (49 vs. 48%, P = 0.87), but a significant lower rate of complications in patients without diabetes treated with intensive compared with conservative treatment regimen (34 vs. 55%, P = 0.008).
Conclusions: Intensive insulin therapy to target glucose of 100 and 140 mg/dL in the ICU did not significantly reduce perioperative complications compared with target glucose of 141 and 180 mg/dL after CABG surgery. Subgroup analysis showed a lower number of complications in patients without diabetes, but not in patients with diabetes treated with the intensive regimen. Large prospective randomized studies are needed to confirm these findings.
Hyperglycemia is common in patients undergoing cardiac surgery, reported in 60-90% of patients with a known history of diabetes and in more than half of patients without diabetes (1,2). Many cohort studies have identified diabetes as an independent risk factor of morbidity and mortality after cardiac surgery (3-5). Patients with diabetes have worse surgical outcomes when compared with those without diabetes, specifically higher mortality, deep sternal wound infections, renal failure, postoperative strokes, longer hospital stays, and higher health care resource utilization (3-7). Similarly, long-term survival after surgical revascularization is significantly reduced in patients with diabetes compared with those without diabetes (7,8).
Several cohort studies as well as prospective clinical trials in cardiac surgery patients have reported that improvement in glycemic control can reduce short- and long-term complications and hospital mortality (9-11). However, several recent randomized trials in mixed intensive care unit (ICU) populations have shown that intensive insulin therapy (glucose target <110 mg/dL) does not reduce complications compared with conventional control but increases the risk of hypoglycemia (12-14). The American Diabetes Association and American Association of Clinical Endocrinologists have recommended maintaining glucose levels between 140 and 180 mg/dL for most ICU patients (15). There is concern that these higher glucose targets may increase the risk of hospital complications in cardiac surgery patients in whom previous randomized trials (9-11) and meta-analyses (14,16) consistently reported that intensive glycemic control reduces perioperative infections, resource utilization, and cardiac-related mortality. In order to determine if the lower end of the recommended glucose target can reduce hospital complications in patients undergoing coronary artery bypass surgery (CABG), we randomized patients with hyperglycemia to an intensive insulin therapy aimed to maintain a blood glucose (BG) level between 100 and 140 mg/dL or to a conservative therapy aimed to maintain a glucose value between 141 and 180 mg/dL in the ICU. The primary outcome of this trial was to determine differences between groups on a composite of hospital complications, including mortality, wound infection, bacteremia, respiratory failure, acute kidney injury, and major cardiovascular events (MACE).
RESEARCH DESIGN AND METHODS
This randomized open-label clinical trial included patients with and without diabetes undergoing primary, elective, and emergency CABG who experienced perioperative hyperglycemia, defined as a BG >140 mg/dL. We recruited patients aged between 18 and 80 years undergoing primary or a combination of CABG and other cardiac operations such as valve repair or aortic surgery. We excluded patients with impaired renal function (serum creatinine >3.0 mg/dL or glomerular filtration rate <30 mL/min/1.73 m2), hepatic failure, or history of hyperglycemic crises and those at imminent risk of death (brain death or cardiac standstill) or pregnancy, or patients or next of kin unable to provide consent. Patients consented during the ambulatory preoperative evaluation visit or on admission to the surgery service. If not performed prior to surgery, patients with hyperglycemia or a legally authorized representative consented within 24 h after surgery. A research pharmacist following a computer-generated block randomization table coordinated randomization and treatment assignment.
Patients assigned to the intensive group received continuous insulin infusion (CII) adjusted to maintain a glucose target between 100 and 140 mg/dL in the ICU. Those assigned to conservative control received CII adjusted to maintain a glucose level between 141 and 180 mg/dL in the ICU. After discontinuation of CII, subjects were transitioned to a single treatment protocol aimed to maintain a glucose target <140 mg/dL before meals during the hospital stay and during the 90 days after discharge (Supplementary Table 2).
This study was conducted at three academic medical centers, including Emory University Hospital, Emory Midtown Hospital, and Grady Memorial Hospital in Atlanta, GA. The institutional review board at Emory University approved the study protocol and consent.
Outcome Measures
The primary outcome was to determine differences between intensive and conservative glucose control on a composite of hospital mortality and perioperative complications, including sternal wound infection (deep and superficial), bacteremia, respiratory failure, pneumonia, acute kidney injury, and MACE (acute myocardial infarction, congestive heart failure, and cardiac arrhythmias).
The secondary outcome was to compare differences between intensive and conservative glucose control on the following: 1) glycemic control, including mean daily and fasting glucose concentration, number of hypoglycemic events (<70 mg/dL) and severe hypoglycemia (<40 mg/dL), and glycemic variability; and 2) individual complications: MACE as defined per the American College of Cardiology–American Heart Association, including acute myocardial infarction, congestive heart failure, and cardiac arrhythmias (17); acute kidney injury, defined as an increment in creatinine level >50% from baseline; respiratory failure, defined as the need for ventilator assistance for longer than 48 h; pneumonia; cerebrovascular events; surgical wound infections recorded as deep sternal wound infection, defined as chest wound infection involving the sternum or mediastinal tissues and as superficial sternal wound infection as those chest wound infections involving the skin or subcutaneous (SC) tissues; mortality was recorded during admission, either during ICU, transition to non-ICU hospital setting, or 90 days after discharge. In addition, we collected information on hospital length of stay (LOS), ICU readmissions, reoperations, and number of hospital readmissions and emergency room visits after discharge.
Insulin Treatment
Hyperglycemia prior to or during surgery was managed according to a standard institutional management protocol. Patients with perioperative glucose >140 mg/dL were randomized after completion of surgery in the post-surgical holding area or in the ICU. Glucommander, a computer-guided CII device, was used to facilitate glycemic control with a single insulin delivery program. The characteristics and use of the Glucommander algorithm have been reported previously (18). In brief, this computer-guided insulin algorithm directs the administration of intravenous insulin in response to glucose measurement at the patient’s bedside. During the infusion, glucose levels were entered into the system and the program recommended the insulin infusion rate and a variable time to check the next glucose testing. Intravenous insulin infusion was continued in the ICU until the patient was able to eat and/or transferred to non-ICU service. After discontinuation of CII, patients with known diabetes were transitioned to SC basal or basal/bolus insulin regimen adjusted daily to achieve and maintain a premeal glucose <140 mg/dL (Supplementary Data).
Statistical Analysis
The study was a two-arm, randomized, multicenter, open-label, controlled, intention-to-treat trial. We conducted nonparametric comparisons of the incidence rates of hospital mortality and perioperative complications based on the two-sided X2 test (or Fisher exact test in the presence of low incidence rates), followed by the Cochran-Mantel-Haenszel test, which adjusts for the potential center effect and the influence of stratification based on diabetes status. Univariate Poisson regression (or negative binomial regression) was performed to assess for the difference in the number of perioperative complications between the two groups.
For the analysis of secondary end points, we used the same statistical strategy planned for the primary end point to analyze secondary end points that yield binary or count outcomes. For secondary end points that produce continuous outcomes, we used two-sample Student t tests or nonparametric Wilcoxon rank sum tests to compare differences between the intensive glucose control group and the conservative glucose control group.
Sample Size Calculation and Power Analysis
We calculated the sample size based on previous studies by van den Berghe et al.(9) and Umpierrez et al. (19). We estimated an incidence rate of the primary end point in the control group of ~20% and odds ratio for the intensive versus conservative glucose control group of ~0.35. We expected a low attrition rate of <10% in the ICU; using two-sided Fisher exact test, with a =0.05, we estimated that the sample size required for 80% power to be 148 patients per group (a total of 296 patients) for the primary end point. For all analyses, reported P values are two-sided, and P values ,0.05 were considered significant. All analyses were performed using SAS software version 9.2 (SAS Institute, Cary, NC).
RESULTS
A total of 855 patients were screened to participate and 338 patients consented. Of them, 33 subjects were excluded because they did not develop hyperglycemia after surgery or withdrew consent for participation (Supplementary Data). A total of 305 patients were randomized; of them, 1 patient in the intensive group and 2 patients in the conservative group withdrew after randomization but prior to receiving insulin treatment. A total of 151 patients in the intensive group and 151 in the conservative group were included in the final analysis. The clinical characteristics of study patients are shown in Table 1. The groups were well balanced with no significant differences in the mean age, racial distribution, BMI, smoking history, history and duration of diabetes, type of treatment prior to admission, or hospital LOS between treatment groups. Most patients underwent primary and isolated CABG surgery; only 19 patients (6.3%) had a previous CABG and 45 patients (14.9%) had combined CABG and valve surgery. The mean number of grafts was 3 + 1 and the duration of surgery was 5.3 + 1.5 h.
Table 1. Clinical characteristics of study patients
| Variable | Conservative | Intensive | P value |
|---|---|---|---|
| Number of Patients | 151 | 151 | |
| Sex | 0.44 | ||
| Male, n (%) | 112 (74) | 106 (70) | |
| Female, n (%) | 39 (26) | 45 (30) | |
| Age (years) | 64 ± 10 | 64 ± 9 | 0.84 |
| Race | >0.99 | ||
| Caucasian, n(%) | 111 (74) | 110 (73) | |
| African American, n(%) | 34 (23) | 35 (23) | |
| Other, n(%) | 6 (4) | 6 (4) | |
| Body weight (kg) | 90.6 ± 21.5 | 93.0 ± 21.4 | 0.47 |
| BMI (kg/m2) | 30.3 ± 7.2 | 31.2 ± 7.2 | 0.40 |
| Past medical history | |||
| Previous smoking, n(%) | 63 (51) | 57 (42) | 0.13 |
| Current smoking, n(%) | 46 (33) | 33 (23) | 0.07 |
| Dyslipidemia, n(%) | 123 (81) | 128 (86) | 0.30 |
| Hypertension, n(%) | 135 (91) | 142 (94) | 0.38 |
| APACHE score | 22.4 ± 3.3 | 21.7 ± 3.6 | 0.12 |
| ASA classification | >0.99 | ||
| Grade 3, n(%) | 10 (7) | 10 (7) | |
| Grade 4, n(%) | 141 (93) | 141 (93) | |
| Surgery | 0.91 | ||
| Elective, n(%) | 24 (16) | 25 (17) | |
| Urgent, n(%) | 126 (83) | 124 (82) | |
| Emergency, n(%) | 1 (1) | 2 (1) | |
| Type of Surgery | |||
| Primary isolated CABG, n(%) | 114 (75) | 123 (81) | 0.22 |
| CABG + valve repair, n(%) | 27 (18) | 18 (12) | 0.15 |
| Redo CABG, n(%) | 10 (7) | 9 (6) | >0.99 |
| History of diabetes, n(%) | 75 (50) | 77 (51) | 0.82 |
| Duration of diabetes (years) | 10.8 ± 10.1 | 10.9 ± 8.8 | 0.72 |
| Admission diabetes therapy | 0.97 | ||
| No antidiabetic agents, n(%) | 5 (7) | 7 (9) | |
| Oral agents, n(%) | 34 (48) | 34 (45) | |
| Insulin alone, n(%) | 14 (20) | 15 (20) | |
| Insulin + oral agents, n(%) | 18 (25) | 20 (26) | |
| ICU LOS (days) | 4.8 ± 10.0 | 3.6 ± 5.0 | 0.09 |
| Hospital LOS (days) | 11.4 ±> 11.0 | 9.5 ± 5.8 | 0.13 |
Data are mean ± SD or n (%). APACHE, Acute Physiology and Chronic Health Evaluation; ASA, American Society of Anesthesiologists.
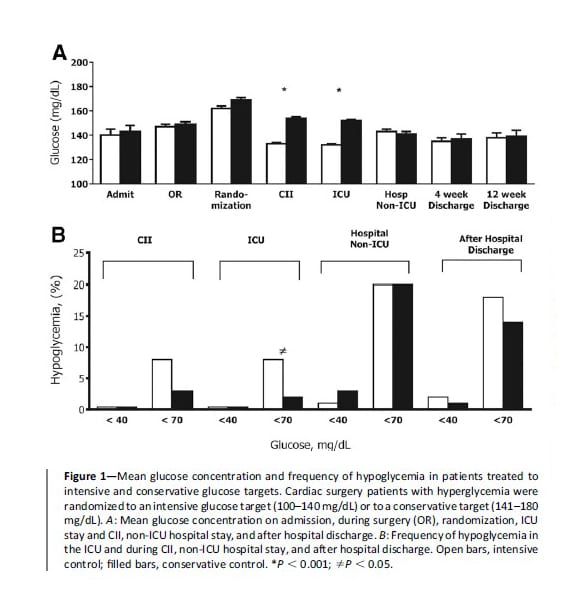
Blood glucose concentration during the hospital stay is shown in Fig. 1A. There were no differences between intensive and conservative groups in the mean glucose on admission, randomization, or during surgery (Table 2). A total of 93% of patients with diabetes and 83% of patients without diabetes developed a glucose >140 mg/dL; of them, 94% of patients with diabetes and 88% of patients without diabetes received CII (P =0.08).The mean BG during the ICU stay was 132 + 14 mg/dL (interquartile range [IQR] 124-139) in the intensive and 154 + 17 mg/dL (IQR 142-164) in the conservative group (P , 0.001). The mean BG concentration during intravenous CII was 133 + 14 mg/dL (IQR 124-139) in patients randomized to the intensive and 154 + 16 mg/dL (IQR 145-164) in the conservative group (P <0.001). The duration of CII was 26.3 + 22 h in the intensive and 22.0 + 24 h in the conservative group (P = 0.001). The total daily dose of insulin during CII was higher in the intensive (36.2 + 42 units/day) compared with the conservative group (29.3 + 46 units/day)(P = 0.008). After discontinuation of CII, 98% of patients with diabetes and 49% of patients without diabetes were transitioned to SC insulin regimen. There were no differences between intensive and conservative groups in mean daily glucose posttransition during the hospital stay (Table 2).
Hypoglycemia (<70 mg/dL) occurred during CII in 12 patients (8%) in the intensive group and 5 patients (3%) in the conservative group during CII (P = 0.13); during the entire ICU stay (off/on CII), a total of 13 patients (9%) in the intensive group and 5 patients (3%) in the conservative group had a glucose <70 mg/dL (P = 0.09) (Table 2). After transferring out of the ICU, a similar frequency of hypoglycemic events was recorded in the intensive and conservative groups during the hospital stay and after hospital discharge (Fig. 2). There were no episodes of severe hypoglycemia in either group in the ICU and only 2% of patients had glucose <40 mg/dL after transitioning out of the ICU. None of the hypoglycemic events was associated with clinically significant adverse outcomes.
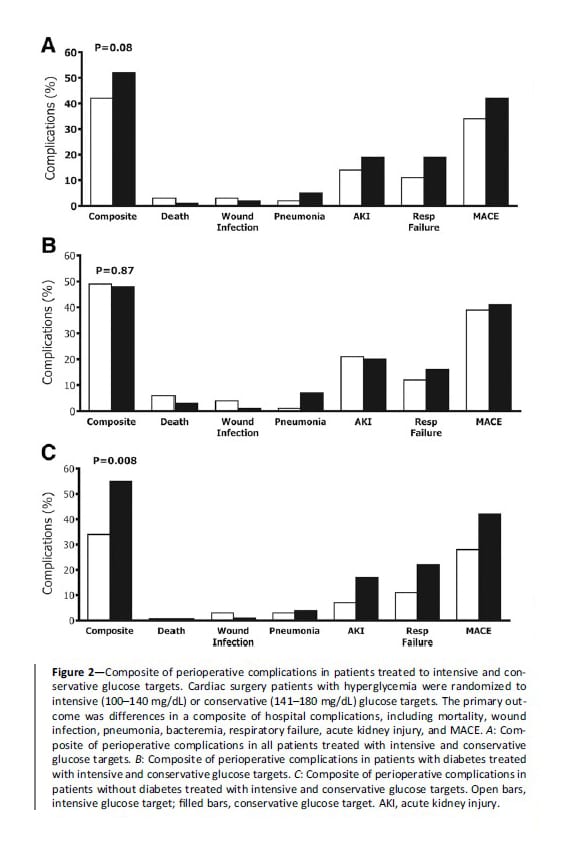
Figure 2A depicts the frequency of the composite and individual complications during the perioperative period. We observed a lower but not significant difference in the number of patients experiencing one or more complications in the intensive compared with the conservative group (42 vs. 52%, P =0.08). There were no differences between groups in the frequency of individual complications, including wound infection, pneumonia, bacteremia, respiratory failure, acute kidney injury, MACE, and death. In addition, we found no differences in the number of ICU readmissions, hospital LOS, or readmissions after hospital discharge (Fig. 2A and Table 2). Figure 2B and C depicts the frequency of composite and individual complications during the perioperative period in patients with and without diabetes treated to intensive and conservative glucose targets.
Table 1. Glycemic control, hypoglycemia, and insulin therapy in patients randomized to intensive and conservative glucose targets
| Variable | Conservative | Intensive | P value |
|---|---|---|---|
| Glycemic control in the ICU | |||
| Admission HbA1c (%) | 6.761.8 | 6.9 ± 1.9 | 0.61 |
| Randomization BG (mg/dL) | 169.0 ± 29.9 | 162.9 ± 24.0 | 0.09 |
| BG during CII (mg/dL) | 154.4 ± 15.9 | 132.5 ± 14.1 | <0.001 |
| BG during ICU stay (mg/dL) | 151.9 ± 16.5 | 132.1 ± 14.1 | <0.001 |
| ICU day 1 (mg/dL) | 154.2 ± 19.9 | 134.9 ± 17.1 | <0.001 |
| ICU day 2 (mg/dL) | 149.6 ± 20.4 | 126.6 ± 16.9 | <0.001 |
| Number of BG readings during CI | 28.2 ± 28.6 | 25.9 ± 30.9 | 0.71 |
| BG readings >200 mg/dL during CII (%) | 7.4 ± 9.9 | 3.4 ± 7.9 | <0.001 |
| BG readings >300 mg/dL during CII (%) | 0.2 ± 1.5 | 0.1 ± 0.8 | 0.25 |
| Glycemic control after ICU | |||
| Hospital BG non-ICU (mg/dL) | 141.3 ± 29.1 | 143.4 ± 27.6 | 0.44 |
| Outpatient BG at 12 weeks postdischarge | 139.4 ± 33.7 | 138.4 ± 26.8 | 0.69 |
| Hypoglycemia during ICU care | |||
| Patients <70 mg/dL during CII, n(%) | 5 (3) | 12 (8) | 0.13 |
| Patients <70 mg/dL during ICU, n(%) | 3 (2) | 13 (9) | 0.09 |
| BG readings during CII <70 mg/dL (%) | 0.1 ± 0.7 | 0.4 ± 2.3 | 0.11 |
| BG readings during ICU <70 mg/dL (%) | 0.1 ± 0.6 | 0.4 ± 2.3 | 0.016 |
| Hypoglycemia after ICU care | |||
| Patients with hospital BG <70 mg/dL after ICU, n(%) | 30 (20) | 30 (20) | >0.99 |
| Patients with BG <70 mg/dL after hospital discharge, n(%) | 20 (14) | 26 (18) | 0.28 |
| Insulin therapy | |||
| Patients treated with CII, n(%) | 133 (88) | 146 (97) | 0.008 |
| Duration of CII (h) | 22.0 ± 24.3 | 26.3 ± 22.2 | 0.001 |
| Total insulin therapy in the ICU (units/day) | 29.3 ± 46.2 | 36.2 ± 42.2 | 0.008 |
| Diabetes management after ICU stay | |||
| Patients transitioned to SC basal or basal bolus insulin, n(%) | 104 (69) | 118 (78) | 0.07 |
| Hospital total SC insulin dose (units/day) | 35.9 ± 34.0 | 42.6 ± 34.8 | 0.11 |
| Patient treated with SC insulin after hospital discharge, n(%) | 47 (31) | 50 (33) | 0.80 |
Data are mean ± SD or n (%).
There were no differences in the overall number of hospital complications between patients with and without a history of diabetes (49 vs. 45%, respectively, P = 0.48). We found, however, significant differences in the effect of intensive compared with conservative insulin therapy on the rate of perioperative complications between patients with and without diabetes. In patients with a history of diabetes, there were no differences in the composite or individual complications in patients treated in the intensive or conservative group (49 vs. 48%, P = 0.87) (Fig. 2B). In contrast, we found that patients without a history of diabetes who were treated in the intensive group experienced a lower number of perioperative complications compared with patients in the conservative group (34 vs. 55%, P = 0.008) (Fig. 2C).
Patients with a history of diabetes were heavier, had higher admission hemoglobin A1c (HbA1c), and had a higher perioperative glucose concentration compared with patients without diabetes (all P <0.05) (Supplementary Data). There were no differences in the number of surgical grafts, duration of surgery, or in the need for vasopressors after surgery between patients with and without a history of diabetes. However, patients with diabetes had a higher mortality (5 vs. 0.5%, P =0.02) and more acute kidney injury (20 vs. 12%, P = 0.048) than subjects without diabetes (Supplementary Fig. 2).
CONCLUSIONS
This randomized controlled trial investigated the risk and benefits of intensive versus conservative insulin therapy in cardiac surgery (CABG) patients. Our study indicates that intensive therapy with a target glucose between 100 and 140 mg/dL in the ICU resulted in a lower, but not significant, reduction in the composite of perioperative complications including mortality, sternal wound infection, bacteremia, respiratory failure, acute kidney injury, and MACE compared with a conservative glucose target between 141 and 180 mg/dL. Although the study was not powered to determine differences in the rate of complications in patients with and without diabetes, we found significant differences in the frequency of complications in patients treated with intensive and conservative insulin therapy in patients without diabetes. Whereas there were no differences between treatment groups in the rate of complications in patients with known diabetes, we observed a significant reduction in complications among patients without diabetes treated in the intensive group compared with those in the conservative group.
During the past decade, there has been ongoing debate about the target goals for optimal glucose control in hospitalized patients with critical illness. Medical organizations involved in the care of patients with diabetes have recommended targeting glucose levels between 140 and 180 mg/dL for the majority of ICU patients, but lower targets between 110 and 140 mg/dL could be appropriate in a select group of ICU patients (i.e., centers with extensive experience and cardiac surgical patients)(15). These recommendations were based on the results of clinical trials in mixed ICU populations with a limited number of cardiac surgery patients that reported high rates of hypoglycemia and lack of improved outcome with intensive insulin therapy (12-14,20). The results of our study indicate a positive trend but not a significant reduction in the rate of peri-operative complications in cardiac surgery patients. Similarly, we observed no differences between intensive and conservative treatment in hospital and ICU LOS, hypoglycemia, need for reoperation, or hospital readmission after discharge.
Several studies have reported that the development of hyperglycemia in patients without a history of diabetes is associated with higher mortality and hospital complications and length of hospital stay compared with patients with diabetes (21-25). A subgroup analysis by van den Berghe et al. (26) of surgical and medical ICU patients reported that whereas glucose lowering effectively reduced mortality in those without a previous history of diabetes, no significant benefit from treatment was observed in patients with diabetes.
However, the NICE-SUGAR (Normoglycemia in Intensive Care Evaluation-Survival Using Glucose Algorithm Regulation) trial reported no differences in complications or mortality between patients with and without diabetes randomized to intensive and conservative insulin therapy (12). Similarly, a recent study by Lazar et al. (27) reported no differences in the composite of complications between intensive and conservative insulin therapy in patients with a history of diabetes. In agreement with van den Berghe et al. (26), we observed a significant reduction in the rate of hospital complications in patients without a history of diabetes treated with intensive glucose control, but not in patients with a previous diagnosis of diabetes. These results indicate that individualization of therapy and glucose targets is needed for the management of patients with hyperglycemia in the perioperative period. In selecting a glucose target, healthcare professionals should consider the level of experience with insulin infusion of the institution, staff support, and risk of hypoglycemia. In addition, our data suggest that a lower glucose target may be appropriate for the patients without diabetes undergoing CABG whereas a higher target may be more appropriate for the patients with preexisting diabetes.
Major strengths of this study include the use of a single glucose control algorithm and the fact that we achieved significant differences in glucose control between groups, which were both within target range. In addition, the rate of hypoglycemia in our study was significantly lower than that observed in previous randomized clinical trials in the ICU. The incidence of severe hypoglycemia, defined as a glucose <40 mg/dL, among the different trials in the ICU has ranged between 5 and 28.6% depending on the intensity of glycemic control (9,12,16,20,28,29). In our trial, using the Glucommander device, only 12 patients (8%) during CII in the intensive group and 5 patients (3%) in the conservative group experienced mild hypoglycemia (<70 mg/dL) and no patients experienced a glucose value <40 mg/dL. Minimizing the rate of hypoglycemia events is of major importance in ICU patients because it has been shown that hypoglycemia may be an independent risk factor of poor clinical outcome and mortality (30-32). In critically ill patients, several studies have shown a strong association between the development of hypoglycemia and an increased risk of cardiovascular events and overall risk of hospital mortality (12,33-35).
We acknowledge several limitations in this trial, including the relatively small sample size. The sample size was calculated based on the results of previous surgical studies (9,19,36) that reported larger reductions in complications between intensive and conservative glucose targets. In this study, we observed a higher rate of complications and a smaller reduction (~20%) in the composite of complications between intensive and conservative treatment groups. Based on the study results, ~800 patients would have been needed to reach power to determine differences in the primary outcome. In addition, the study was conducted at three medical centers with extensive experience in inpatient management of hyperglycemia and we used a computerized insulin infusion device to manage patients in the ICU; thus the findings cannot be generalized to all institutions with less clinical experience or nursing support. In addition, we excluded patients admitted with clinically relevant hepatic and kidney disease or patients with known diabetes receiving corticosteroids or CII prior to surgery. Another limitation is that the study was not powered to demonstrate differences in mortality between treatment groups or difference in complications between patients with and without a history of diabetes.
In summary, intensive control targeting a glucose level between 100 and 140 mg/dL in the ICU did not significantly reduce perioperative complications, mortality, or hospital LOS compared with a less strict glucose target of 141-180 mg/dL in patients undergoing CABG surgery. However, we observed heterogeneity in treatment effect according to diabetes status, with no differences in complications among patients with diabetes, but lower rates of complications in subjects without diabetes treated with intensive compared with conservative regimen.
Funding. This investigator-initiated study was supported by a clinical research grant from the American Diabetes Association (7-03-CR-35) and a grant from the Clinical and Translational Science Award program, National Institutes of Health, National Center for Research Resources (UL1 RR025008). G.U. is supported in part by research grants from the American Diabetes Association (1-14-LLY-36) and a PHS grant from the Clinical and Translational Science Award Program (M01 RR-00039), National Institutes of Health, National Center for Research Resources (UL1 RR025008).
The sponsors of the study were not involved in the study design, data collection, analysis or interpretation of the results, or preparation of the manuscript.
Duality of Interest. This work was supported by an unrestricted grant to Emory University from Sanofi (Bridgewater, NJ). G.U. has received unrestricted research support for inpatient studies (to Emory University) from Sanofi, Merck, Novo Nordisk, Boehringer Ingelheim, Eli Lilly and Company, and Endo Barrier and has received consulting fees or/and honoraria for membership in advisory boards from Sanofi, Merck, and Boehringer Ingelheim. D.S.B. has received research support (to Emory University) from Abbott, Merck, and Sanofi and has received consulting fees or/and honoraria for participation in advisory committees from Janssen, Sanofi, and Boehringer Ingelheim. R.A.G. has received honoraria for consulting work from Medtronic, Inc. No other potential conflicts of interest relevant to this article were reported.
Author Contributions. G.U. wrote the initial research proposal and manuscript. S.C. and M.U. collected and researched the data. F.P., S.J., C.A.N., D.S.B., P.V., M.H., J.D.P., R.A.G., and V.H.T. reviewed and edited the research proposal and manuscript and contributed to the discussion. L.P. conducted the statistical analyses. G.U. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Prior Presentation. This study was presented at the 74th Scientific Sessions of the American Diabetes Association, San Francisco, CA, 13-17 June 2014.
AFFILATIONS
- Department of Medicine, Emory University, Atlanta, Georgia.
- Rollins School of Public Health, Emory University, Atlanta, Georgia.
- Joseph B. Whitehead Department of Surgery, Emory University, Atlanta, Georgia.
REFERENCES
- McAlister FA, Man J, Bistritz L, Amad H, Tandon P. Diabetes and coronary artery bypass surgery: an examination of perioperative glycemic control and outcomes. Diabetes Care 2003; 26:1518-1524.
- Schmeltz LR, DeSantis AJ, Thiyagarajan V, et al. Reduction of surgical mortality and morbidity in diabetic patients undergoing cardiac surgery with a combined intravenous and subcutaneous insulin glucose management strategy. Diabetes Care 2007;30:823-828.
- Carson JL, Scholz PM, Chen AY, Peterson ED, Gold J, Schneider SH. Diabetes mellitus increases short-term mortality and morbidity in patients undergoing coronary artery bypass graft surgery. J Am Coll Cardiol 2002;40:418-423.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003;125:1007-1021.
- Thourani VH, Weintraub WS, Stein B, et al. Influence of diabetes mellitus on early and late outcome after coronary artery bypass grafting. Ann Thorac Surg 1999;67:1045-1052.
- Herlitz J, Wognsen GB, Karlson BW, et al. Mortality, mode of death and risk indicators for death during 5 years after coronary artery bypass grafting among patients with and without a history of diabetes mellitus. Coron Artery Dis 2000;11:339-346.
- Guvener M, Pasaoglu I, Demircin M, Oc M. Perioperative hyperglycemia is a strong correlate of postoperative infection in type II diabetic patients after coronary artery bypass grafting. Endocr J 2002;49:531-537.
- Mathew V, Holmes DR. Outcomes in diabetics undergoing revascularization: the long and the short of it. J Am Coll Cardiol 2002;40:424-427.
- van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med 2001;345:1359-1367.
- Lazar HL, Chipkin SR, Fitzgerald CA, Bao Y, Cabral H, Apstein CS. Tight glycemic control in diabetic coronary artery bypass graft patients improves Perioperative outcomes and decreases recurrent ischemic events. Circulation 2004;109:1497-1502.
- Kitabchi AE, Freire AX, Umpierrez GE. Evidence for strict inpatient blood glucose control: time to revise glycemic goals in hospitalized patients. Metabolism 2008;57:116-120.
- Finfer S, Chittock DR, Su SY, et al.; NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Engl J Med 2009;360:1283-1297.
- Preiser JC, Devos P, Ruiz-Santana S, et al. A prospective randomised multi-centre controlled trial on tight glucose control by intensive insulin therapy in adult intensive care units: the Glucontrol study. Intensive Care Med 2009;35:1738-1748.
- Griesdale DE, de Souza RJ, van Dam RM, et al. Intensive insulin therapy and mortality among critically ill patients: a meta-analysis including NICE-SUGAR study data. CMAJ 2009;180:821-827.
- Moghissi ES, Korytkowski MT, DiNardo M, et al.; American Association of Clinical Endocrinologists; American Diabetes Association. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care 2009;32:1119-1131.
- Wiener RS, Wiener DC, Larson RJ. Benefits and risks of tight glucose control in critically ill adults: a meta-analysis. JAMA 2008;300:933-944.
- Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined, a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol 2000;36:959-969.
- Davidson PC, Steed RD, Bode BW. Glucommander: a computer-directed intravenous insulin system shown to be safe, simple, and effective in 120,618 h of operation. Diabetes Care 2005;28:2418-2423.
- Umpierrez GE, Smiley D, Jacobs S, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care 2011;34:256-261.
- Arabi YM, Dabbagh OC, Tamim HM, et al. Intensive versus conventional insulin therapy: a randomized controlled trial in medical and surgical critically ill patients. Crit Care Med 2008;36:3190-3197.
- Falciglia M, Freyberg RW, Almenoff PL, D’Alessio DA, Render ML. Hyperglycemia related mortality in critically ill patients varies with admission diagnosis. Crit Care Med 2009;37:3001-3009.
- Mendez CE, Mok KT, Ata A, Tanenberg RJ, Calles-Escandon J, Umpierrez GE. Increased glycemic variability is independently associated with length of stay and mortality in noncritically ill hospitalized patients. Diabetes Care 2013;36:4091-4097.
- Frisch A, Chandra P, Smiley D, et al. Prevalence and clinical outcome of hyperglycemia in the perioperative period in noncardiac surgery. Diabetes Care 2010;33:1783-1788.
- Kotagal M, Symons RG, Hirsch IB, et al.; SCOAP-CERTAIN Collaborative. Perioperative hyperglycemia and risk of adverse events among patients with and without diabetes. Ann Surg 2015;261:97-103.
- Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab 2002;87:978-982.
- van den Berghe G, Wouters PJ, Kesteloot K, Hilleman DE. Analysis of healthcare resource utilization with intensive insulin therapy in critically ill patients. Crit Care Med 2006;34:612-616.
- Lazar HL, McDonnell MM, Chipkin S, Fitzgerald C, Bliss C, Cabral H. Effects of aggressive versus moderate glycemic control on clinical outcomes in diabetic coronary artery bypass graft patients. Ann Surg 2011;254:458-463.
- Brunkhorst FM, Engel C, Bloos F, et al.; German CompetenceNetwork Sepsis (SepNet). Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med 2008;358:125-139.
- van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med 2006;354:449-461.
- Kagansky N, Levy S, Rimon E, et al. Hypoglycemia as a predictor of mortality in hospitalized elderly patients. Arch Intern Med 2003;163:1825-1829.
- Stagnaro-Green A, Barton MK, Linekin PL, Corkery E, deBeer K, Roman SH. Mortality in hospitalized patients with hypoglycemia and severe hyperglycemia. Mt Sinai J Med 1995;62:422-426.
- Turchin A, Matheny ME, Shubina M, Scanlon JV, Greenwood B, Pendergrass ML. Hypoglycemia and clinical outcomes in patients with diabetes hospitalized in the general ward. Diabetes Care 2009;32:1153-1157.
- Egi M, Bellomo R, Stachowski E, et al. Hypoglycemia and outcome in critically ill patients. Mayo Clin Proc 2010;85:217-224.
- Krinsley JS, Grover A. Severe hypoglycemia in critically ill patients: risk factors and outcomes. Crit Care Med 2007;35:2262-2267.
- Preiser JC, Brunkhorst F. Tight glucose control and hypoglycemia. Crit Care Med 2008;36:1391; author reply 1391-1392.
- Halkos ME, Puskas JD, Lattouf OM, et al. Elevated preoperative hemoglobin A1c level is predictive of adverse events after coronary artery bypass surgery. J Thorac Cardiovasc Surg 2008;136:631-640.