Relationship Between Glycemic Control Using eGMS and Readmission Rates in Cardiovascular Patients Hospitalized with AMI, CHF or Undergoing CABG During the Implementation of a System Wide Glycemic Initiative
![]()
Presentation
Annual Diabetes Technology Meeting
Date
November 2016
Authors
April Mumpower,1 Suqin Hou,2 Tamera Parsons,1 Raymie McFarland2
OBJECTIVE
The CMS Hospital Readmission Reduction (HRR) program was initiated in 2012 to encourage hospitals to implement quality improvement programming to reduce the rate of readmissions through a hospital financial penalty. Uncontrolled inpatient hyperglycemia has been associated with increased readmission rates. Normoglycemia has been associated with improved patient outcomes, including decreased mortality, complications, length of stay and readmissions. This study evaluated the readmission outcomes of patients using an Electronic Glycemic Management System (eGMS) Glucommander (GM) for inpatient insulin management versus Standard Care (SC) in patients with Acute Myocardial Infarction (AMI), Congestive Heart Failure (CHF) and those undergoing Coronary Artery Bypass Grafting (CABG) procedures.
METHODS
This retrospective study evaluated 3198 patients with AMI, CHF or undergoing a CABG procedure who were admitted to a 13 hospital health system over a 12 month time frame from January 2015 through December 2015. Qualifying patients were treated with eGMS IV and/or SubQ insulin management or those treated by SC. The main outcome measure was Risk Adjusted Readmission Rates.
RESULTS
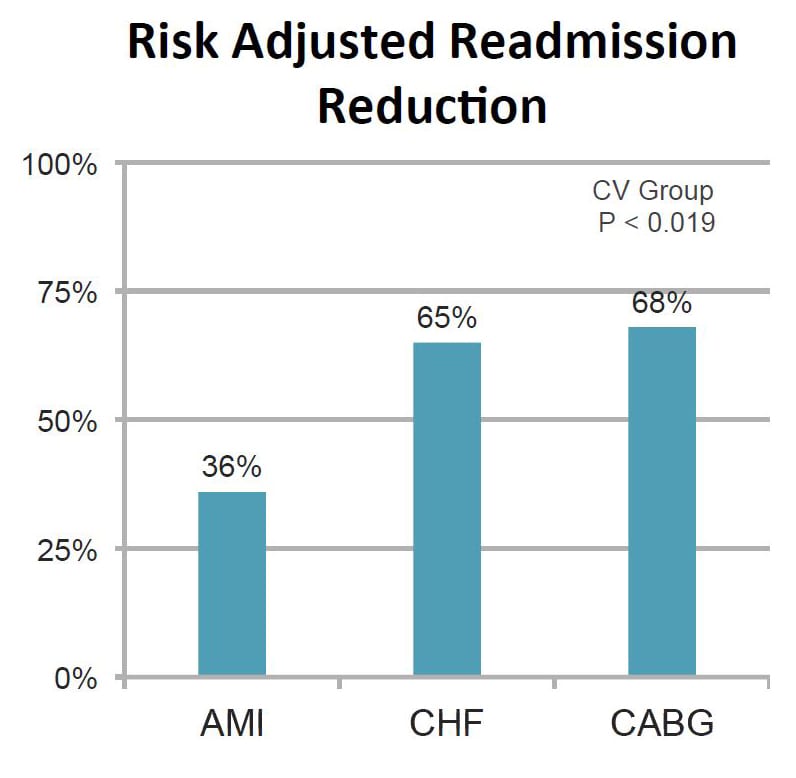
Patients (n=281) treated with eGMS had a Risk Adjusted Readmission rate of 0.75 for AMI, 0.34 for CHF and 0.65 for CABG. Patients (n=2917) treated with SC had a Risk Adjusted Readmission rate of 1.17 for AMI, 0.97 for CHF and 2.04 for CABG. The p values from the t-tests of the observed cardiac patient groups (p=0.019 SD 2.990, 2.618) determined statistical 95% significance p <0.05, particularly for CHF (p <0.009 SD 1.993, 0.905). Patients treated with eGMS had a reduced Risk Adjusted Readmission rate of 36% for AMI, 65% reduction for CHF and 68% for CABG.
| Patient Characteristics | eGMS | Standard Care | p Value |
|---|---|---|---|
| Average Admission Blood Glucose | 241.5 mg/dL (SD = 185.8) | 237.6 mg/dL (SD = 143.8) | 0.56 |
| Average Blood Glucose | 136.1 md/gL (SD = 64.2) | 176.5 mg/dL (SD = 79.4) | <0.0001 |
| Average Final Blood Glucose | 122.1 mg/dL (SD = 43.0) | 184.1 mg/dL (SD = 68.8) | <0.0001 |
| % of Blood Glucose Events Hypoglycemia <40 mg/dL | 0.01% | 0.39% | <0.0001 |
| % of Blood Glucose Events Hyperlgycemia <70 mg/dL | 0.50% | 2.78% | <0.0001 |
| % of Blood Glucose Events Hyperglycemia >180 mg/dL | 9.14% | 38.3% | <0.0001 |
| % of Blood Glucose Events in Target Range 70-180 mg/dL | 90.3% | 58.9% | <0.0001 |
| % of Patients Hypoglycemia <40 mg/dL | 0.52% | 7.58% | <0.03 |
| % of Patients Hypoglycemia <70 mg/dL | 12.0% | 29.4% | <0.0001 |
| Risk-Adjusted Readmission Rate | eGMS | Standard Care |
|---|---|---|
| Number of Patients | 281 | 2,917 |
| AMI | 0.75 | 1.17 |
| CHF | 0.34 | 0.97 |
| CABG | 0.65 | 2.04 |
CONCLUSION
The evidence presented in these results suggest that glycemic control using eGMS can effectively reduce the rate of readmission for patients with cardiovascular disease who are in need of insulin management. There is enough evidence supporting a decrease in risk-adjusted readmission rates among groups treated with eGMS management.
Affiliations
- Mountain States Health Alliance, Johnson City, Tennessee.
- Glytec, Waltham, Massachusetts.