Use of a Computerized Intravenous Insulin Algorithm Within a Nurse-Directed Protocol for Patients Undergoing Cardiovascular Surgery
![]()
Publication
Journal of Diabetes Science and Technology
Date
May 2008
Authors
Paul Davidson,1 R Dennis Steed,2 Bruce Bode,1 Harry Hebblewhite,1 Louis Prevosti,3 Vasundhara Cheekati4
Abstract
Background: Several studies have shown the benefits of tight glycemic control in intensive care unit. A large hospital became concerned about certain deficiencies in the management of glucose control in conjunction with cardiovascular surgery. A multidisciplinary steering committee was formed, which implemented a glycemic protocol, the subject of this study.
Methods: The glycemic control is a perioperative, nurse-directed program that incorporates the computerized intravenous (IV) insulin algorithm, Glucommander. Upon admission, hemogoblin A1c and blood glucose (BG) were tested, and patients were screened for previously diagnosed diabetes. This information was used to determine if preoperative insulin will be used, if the patient will be transitioned post-IV to subcutaneous (SC) basal-bolus insulin, and if insulin will be prescribed on discharge. IV insulin was initiated perioperatively in known diabetes cases or if one BG value >140 mg/dl or two BG values >110mg/dl within 24 hours before or during surgery. The target range was 90 to 120 mg/dl.
Results: In the 9 months after protocol implementation, 93% of the patients had no BG value >200 mg/dl during the first 48 hours postoperatively. In the 6 months of study data, there were 457 patients. The mean time to target range was 3.0 hours. The mean IV insulin run time was 37 hours. The mean BG value was 107 mg/dl. Only 2% of patients had transient BG <50 mg/dl, and no BG values were <40 mg/dl. Of the patients, 52% were transitioned to SC basal-bolus, and 26% were discharged on insulin.
Conclusions: The Glucommander earned high respect from the nurses for the way it scheduled BG tests and eliminated the calculation time and calculation errors associated with manual methods. The protocol was highly effective in normalizing glucose without hypoglycemia. The multidisciplinary steering committee proved to be a good approach to implementing a glycemic protocol.
Introduction
Numerous studies to date have shown the benefits and also the risks of tight glycemic control in the hospital, specifically in the intensive care unit (ICU).1-3 Tight control usually requires complex insulin dosing regimens that are restricted to the ICU due to the need for a skilled, highly trained staff of nurses who are responsible for only one or two patients at a time. Severe hypoglycemia is a concern with many intravenous (IV) insulin protocols and, in at least one study, has been shown to be an independent risk factor for mortality.4 This article discusses the methods, results, and benefits of a nurse-directed, computerized protocol in patients undergoing coronary bypass or valve surgery.
The recommended goals for glycemic control in the hospital vary slightly. In the ICU, both the American Association of Clinical Endocrinologists (AACE) and the American Diabetes Association (ADA)5 recommend <110 mg/dl in the general medical-surgical units, AACE recommends <110 mg/dl premeal and peak postprandial <180 mg/dl, whereas ADA recommends 90 to 130 mg/dl premeal. According to ACE/ADA guidelines,5 components of the optimum strategy for achieving improved management of diabetes in hospitalized patients consist of the following.
- An appropriate level of administrative support.
- Formation of a multidisciplinary steering committee to promote the development of initiatives.
- Assessment of current processes, quality of care, and barriers to necessary changes in practice.
- Development and implementation of interventions, including standardized order sets, protocols, policies, and algorithms, with associated educational programs.
- Metrics for evaluation.
In August 2005, prior to the institution of these guidelines at Piedmont Hospital in Atlanta, Georgia, postcoronary bypass patients received IV boluses of sliding scale insulin, there were rare endocrine consults, and the patients were in generally poor glucose control. One of the authors (P.C.D.), an endocrinologist on staff, wrote a report detailing the poor glycemic control in a post bypass type 1 patient with diabetes and offered a working protocol recommending a more aggressive diabetes management plan based on a computerized algorithm. At the time of this appeal, Piedmont Hospital had already joined the 100,000 Lives Campaign of Institute for Healthcare Improvement (IHI).6 An analysis of the preceding 5 months revealed that only 54% of the cardiovascular (CV) patients had met the IHI initiative of all blood glucose values being <200 mg/dl in the first 48 hours postsurgery. Within days after circulating the report, the cardiothoracic surgeons and ICU administration sanctioned the formation of a steering committee and agreed to support it.
The Piedmont Steering Committee was multidisciplinary, composed of persons from thoracic surgery, endocrinology, nursing (ICU and step-down), pharmacy, the diabetes treatment center, nutrition, and the heart center. The focus was limited to cardiothoracic surgery only. It was recognized that the burden of carrying out the protocol would fall on nurses.
Methodology
Based on the aforementioned goals, the Piedmont Steering Committee decided to implement a nurse-directed tight glycemic control protocol for patients undergoing coronary bypass and valve surgery. In order to accomplish this task, the committee met weekly over a 5-month period to develop such a protocol. A protocol was agreed upon and initiated in February 2006. Since then all cardiovascular surgery (CVS) patients have been included. The specifics of the protocol are as follows:
Glycemic Protocol
- The protocol is nurse-directed so that all patients are treated uniformly.
- For all patients, hemoglobin A1c and glucose are tested on arrival. Hemoglobin A1c is used to guide post-IV therapy, including the duration of IV insulin, the need for SC after IV insulin, and the need for insulin therapy upon discharge.
- If a patient is admitted on the day before surgery and the hemoglobin A1c is >6%, or if the premeal BG is >140 mg/dl, or if the patient is known to have diabetes, then a weight-based basal-bolus SC insulin regimen is initiated, followed by IV insulin overnight preoperatively.
- Intravenous insulin delivery using the Glucommander is initiated as described earlier for anyone with one BG value >140 mg/dl or two BG values >110 mg/dl within 24 hours before or during surgery. Targets for glucose control are 90 to 120 mg/dl. All glucose values in the ICU are monitored from arterial blood using Abbott meters.
- Hypoglycemia (<60 mg/dl) is treated only with IV 50% dextrose based on formula that is calculated to not overshoot the target range of 90 to 120 mg/dl.7
- The IV insulin therapy is continued until the morning of postoperative day (POD) #1 if hemoglobin A1c <6% and to POD #2 in persons with known diabetes or hemoglobin A1c >6%.
- Post-ICU transition to SC insulin is conducted for all patients with preexisting diabetes or hemoglobin A1c >6%. The SC dosing is based on the patient’s IV insulin requirement. The glargine basal insulin is started at about 9:00 p.m. the night before IV insulin is stopped.
- Endocrine consultation is obtained for any patient with a BG value <70 or >140 mg/dl or for any patient on basal-bolus insulin.
- Discharge planning with diabetes education is initiated for all patients with hemoglobin A1c >7%. Patients with hemoglobin A1c <7% are discharged on preadmission therapy.
Intravenous phase. The Glucommander is a computer guided insulin infusion system invented by Davidson and Steed in 1984.8 Insulin is administered by the following formula: insulin units/hour = multiplier x (BG – BGref). BGref is a reference value, set at 60 mg/dl. The multiplier is adjusted by the computerized algorithm if the blood glucose is not approaching the target range (e.g., 90 to 120 mg/dl), which is input by the nurse at the start of the Glucommander, independently of BGref. There is a variable time interval between blood glucose checks, based on stability of the glucose level. An alarm reminds the nurses when to recheck the glucose level and enter it into the Glucommander, which calculates a new insulin infusion rate and stores data.
Subcutaneous basal-bolus treatment, pre-IV. For total daily dose of insulin (TDD), a weight-based formula is used preoperatively and prior to the Glucommander: weight in kilogram x 0.5 = TDD. Fifty percent of this is basal, given as glargine at bedtime. The remaining 50% of TDD is given as three premeal doses of rapid-acting insulin (RAI), resulting in one-sixth of TDD for each meal. Bedside capillary glucose (BG) is tested premeal, at bedtime, and at 0300, with a correction dose of RAI given for a BG value >140 mg/dl. The correction formula is (BG – 100) divided by the correction factor. The correction factor (CF) is determined by the 1700 rule (1700 divided by the known or estimated TDD).9
Subcutaneous basal-bolus treatment, post-IV. The method for transition from the Glucommander to basal-bolus insulin therapy in this protocol is applied to all patients with known diabetes or hemoglobin A1c >6%. Formulae for the transition are predicated on BGref = 60 mg/dl and a concurrent IV drip of 10% glucose at 50 cc/hr. The transition is made (at 9 pm) if the patient’s BG has been in the target range for three consecutive BG tests and if the multiplier has been stable for three consecutive BG tests. The multiplier is used for the transition calculations as follows:
- Basal Insulin (glargine): Multiplier * 500
- Correction Bolus (aspart): (BG – 100) * Multiplier/1.7
- Meal Bolus (aspart): Multiplier * 167
- Carbohydrate-to-Insulin Ratio (CIR) (aspart): 0.45/Multiplier
The transition is initiated by the nurse. Post-transition, a consulting endocrinologist monitors and confirms each patient’s insulin dosing. SC insulin doses are adjusted by ~20% if BG readings are outside the 70- to 140-mg/dl range. The diet is initially an 1800-kcal ADA diet in all patients, with subsequent adjustment based on nutritional consultation.
Data Collection
Intravenous phase, Glucommander. The program is installed in a Palm device at each patient’s bedside. In the process of operation, the Glucommander records time, BG, multiplier, and IV insulin infusion rate. This information is available by downloading. Immediately after down loading from the Palm device and inserting in the patient’s medical record, personal identifying information was removed from data.
Subcutaneous phase. The manual BG meter automatically downloads to the hospital mainframe computer when placed in the charging stand, making time-logged BG values available from the computer. Administration of SC insulin and doctor’s orders are also available from the computer. Immediately after downloading from the hospital mainframe for placing into the study’s database, all personal identifying data were deleted.
Reassurances that Health Insurance Portability and Accountability violations did not occur. All interactions and data collection were done by one of the authors (P.C.D.) as a requisitioned medical consultation. No institutional review board approval was indicated. All identifiers of individual patients were stripped from the records prior to analysis. Permission to include patients in this study was not necessary, as the activities and collected information were part of routine quality medical care.
Statistical Methods
Our study was compared to Piedmont’s pre-protocol calendar period as follows: From the hospital’s mainframe computer, the following data were extracted. For the period of 5 months prior to the protocol, counts were obtained for patients with no BG value >200 for the first 48 hours after surgery and for patients with at least one BG value >200 for the first 48 hours after surgery. For the period of 9 months after implementation of the protocol, the same data were obtained. We did not remove any personal identifying data from the hospital’s mainframe computer. These four groups were analyzed by a X2 test, as they were count data.
Results
As of December 2007, over 1800 patients have been treated by this protocol with no exceptions. Detailed data were collected for the first 457 patients, who were analyzed in this retrospective study. Results are as follows.
- All CVS patients were treated by the protocol. The description of the sample of patients at admission is shown in Table 1. The protocol enabled easy determination of stage-by-stage treatment regimens during the patients’ hospital stays and at discharge, as also shown in Table 1.
- On IV insulin, the mean time to <120 mg/dl was 3.0 hours. IV insulin was continued for a mean of 37 hours. Mean BG was 107 mg/dl, 7.7% of patients had a BG value <60 mg/dl, 2% of patents had transient BG value <50 mg/dl, and no patient had a BG value <40 mg/dl (see Table 2).
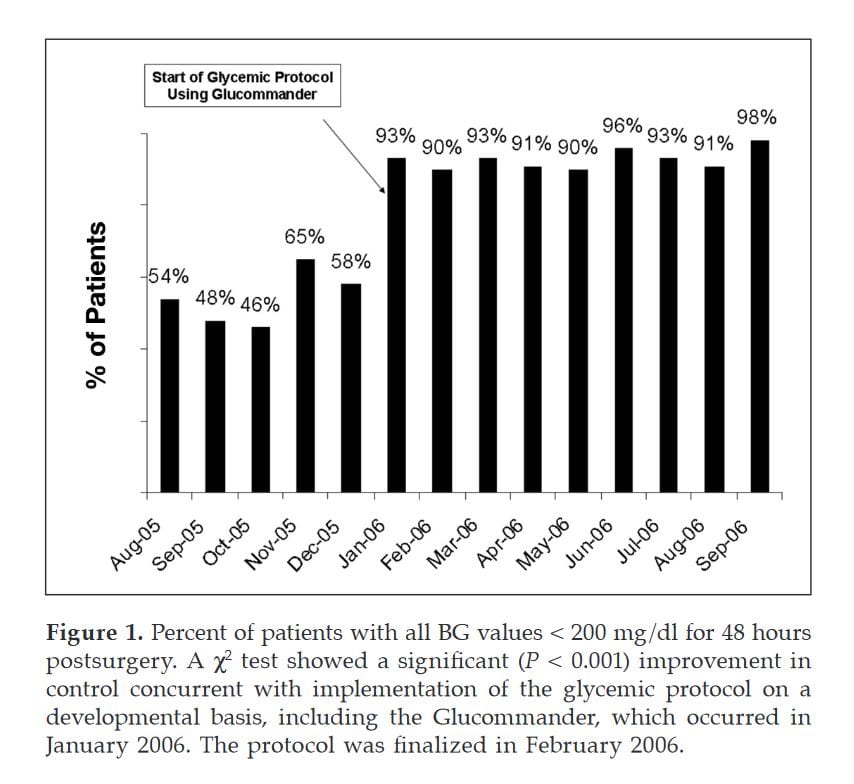
- In the 9 months after the initiation of the protocol, 93% of patients were well controlled to a degree that no BG value was >200 mg/dl during the first 48 hours postoperatively (see Figure 1). This compares to 54% during the 5-month period before the inception of the protocol. The accompanying count data were as follows: In the 5 months before the initiation of the protocol there were 176 patients with no BG value >200 mg/dl and 149 patients with at least one BG value >200. In the 9 months after initiation of the protocol there were 543 patients with no BG value >200 and 42 patients with at least one BG value >200 mg/dl. A X2 test gave a significant result (P <0.001).
- The results of glucose levels in various ranges are shown in Table 2. For comparison, the percentage of glucoses less than 40 mg/dl in Leuven data was 5.2%.1
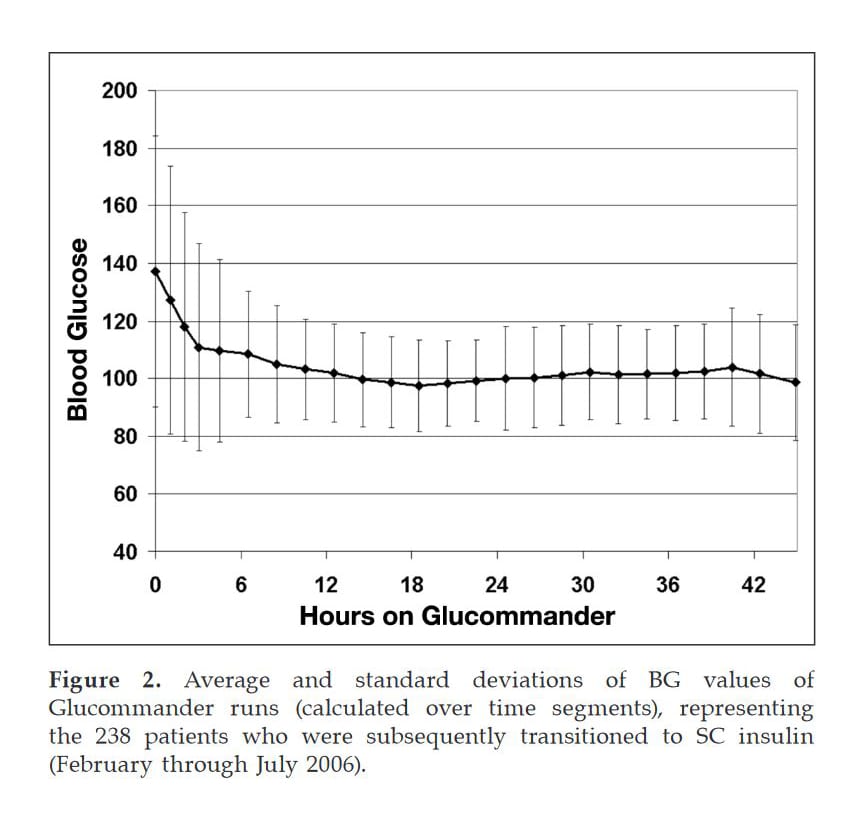
- Figure 2 shows a graph of mean glucose level vs time achieved with the Glucommander for patients with previously diagnosed diabetes mellitus (DM) or hemoglobin A1c >6%, before transition to SC.
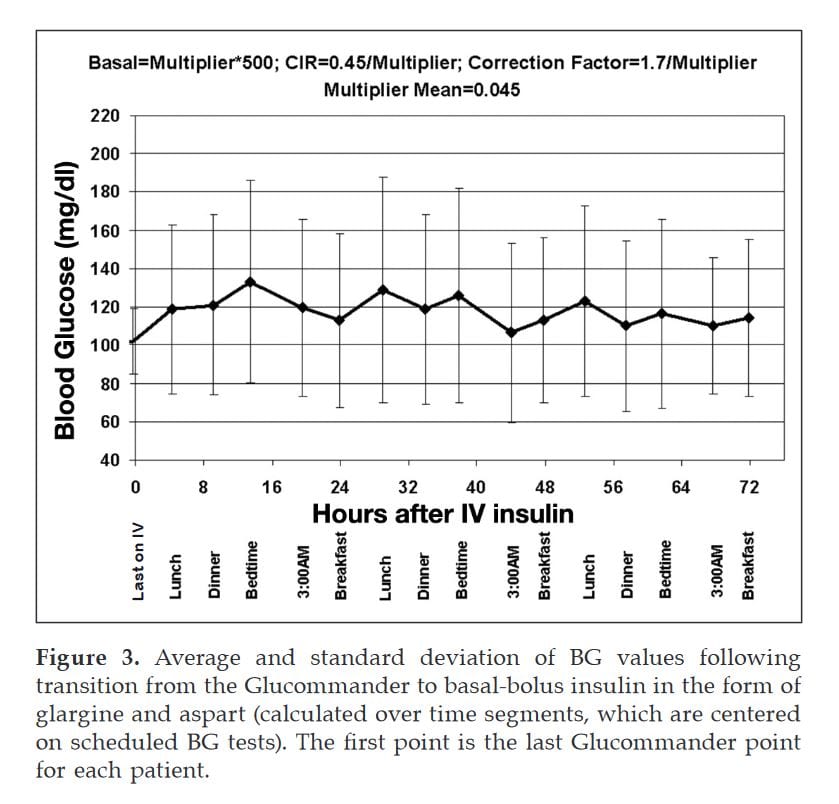
- All patients with previously diagnosed DM or hemoglobin A1c >6% were transitioned to SC basal-bolus (52% of patients). Figure 3 shows a graph of mean blood glucose vs time achieved with basal-bolus after transition from IV.
- The average multiplier at transition was 0.045 (range 0.016-0.183). From this, the average basal = 0.045 * 500 = 22.5 units (range 8-92), the average meal bolus = 0.045 * 167 = 7.5 units (range 3-31), the average CIR = 0.45/ 0.045 = 10 grams of carbohydrate/unit (range 2.5-28), and the average CF = 1.7/0.045 = 38 (range 9-106).
- In post-transitioned data, only 0.4% of the BG values were <50 mg/dl and only 4.9% were >200.
- Nursing acceptance is uniformly enthusiastic. The only initial complaint was the increased frequency of glucose monitoring while on IV insulin. This complaint subsided once the nurses observed the optimal control and the infrequency of needing to call for order changes. Because of Glucommander prompting, nurses were able to follow the protocol within their first shift on the CV ICU postoperative unit or CV floor. Surgeons’ acceptance of the protocol has been positive with no complaints.
Table 1. Description of Sample of Patients at Admission and Stage by Stage through Hospital Stay to Discharge
| Patients at Admission | |
|---|---|
| Average Age | 63 ± 11 |
| Average Weight (kg) | 88 ± 26 |
| Average Body Mass Index | 30 ± 8 |
| Sex | |
| Male | 70% |
| Female | 30% |
| At Admission | |
| % on Insulin | 10 |
| % with Previously Diagnosed DM | 28 |
| % with Hemogloblin A1c >6 | 48 |
| % with Any of the Above | 52 |
| % Patients Admitted on Oral Hypoglycemia Agents | 21 |
| Oral Hypoglycemia Agent Types (% of Patients on OHA) | |
| Meglitinides | 1 |
| Sulfonylurea | 10 |
| Biguanides | 58 |
| Thiazoiidinediones | 33 |
| Decisions by Protocol | |
| Percentage Given Postoperative IV Insulin | 96 |
| Percentage Given Post-IV Basal-Bolus Insulin | 52 |
| Percentage Discharged on Insulin | 26 |
| All patients had been on post-IV basal-bolus; all were discharged on basal-bolus. | |
Table 2. Blood Glucose Results for Varied BG and Time Ranges Encompassing Postoperative IV Insulin and Subcutaneous Insulin*
| BGs | Glucommander >4 hr | Post-Glucommander | ||||
|---|---|---|---|---|---|---|
| N | 2967 | 2920 | ||||
| Mean | 103 mg/dl | 122 mg/dl | ||||
| SD | 19 | 40 | ||||
| BGs | No. | % BG | % Pts | No. | % BG | % Pts |
| >200 | 4 | 1.3 | 14.3 | 142 | 4.9 | 28 |
| <60 | 10 | 0.34 | 7.7 | 45 | 1.6 | 14 |
| <50 | 3 | 0.1 | 2 | 13 | 0.4 | 6 |
| <40 | 0 | 0 | 0 | 2 | 0.1 | 1.3 |
| *Ninety-eight percent of BG values remained in the 60- to 200-mg/dl range while on the Glucommander. For comparison with the table, the percentage of patients with any BG <40 mg/dl in the surgical ICU at the University of Leuven was 5.2%.1 | ||||||
Discussion
In most hospitals, transition is a vulnerable point for losing control over intensive insulin therapy. From the 11-fold variation in final multipliers reported earlier, it can be seen that the variation in insulin sensitivity (affecting the basal insulin, CF, and CIR) is so great that without some individualized index of insulin sensitivity, such as use of the Glucommander multiplier employed herein, it would be difficult to transition patients quickly and smoothly from IV insulin to glycemic control with basal-bolus insulin.
For non-Glucommander IV algorithms, the average insulin infusion rate can be used as follows: TDD = 8 x [sum of last three insulin infusion rates]. The authors believe that transition formulae from IV to SC insulin described herein are the most valuable new contribution of this protocol.
Conclusions
This nurse-directed, glycemic protocol utilizing a computerized system for IV insulin infusion and transition to SC basal-bolus insulin therapy was highly effective in normalizing glucose without significant hypoglycemia in all patients undergoing CV surgery at Piedmont Hospital in Atlanta. Several important factors were involved in the success of this project. Foremost, the design and implementation of the protocol were by a group effort of diabetes specialists, nurses, pharmacists, and educators under the guidance of a CV surgeon, who sold the program to his fellow surgeons and the hospital administration. Empowerment of the nurses in the design, ownership, and application of the protocol was crucial. The use of a well-researched and proven computerized algorithm for IV insulin dosing (Glucommander) was a factor in the ease of convincing the CV unit and the hospital to undertake this upgrade of glucose management. The appropriate setting of the target range of 90 to 120 mg/dl allowed all patients to obtain a mean glucose value of 107 mg/dl with no glucose value <40 mg/dl. Nurse-directed transition from IV to SC insulin in all patients with known diabetes or a hemoglobin A1c >6% allowed normalization of glucose with eating during the postoperative period and until discharge. The Glucommander protocol was initiated immediately on all patients so there was no delay waiting for an endocrin consult. In order to accomplish this task, all patients on admission had to be screened for diabetes and have a hemogloblin A1c drawn to aid in knowing which patients needed transition from IV to SC insulin and which patients would benefit from insulin upon discharge. In addition, all patients admitted with poorly controlled diabetes was normalized in the hospital with insulin and discharged with an insulin regiment that would keep glucose near normal. It is felt by all team members that a similar glycemic protocol could also be used in normalizing glucose in all other patients in the hospital system. This is now being initiated.
Abbreviations
(AACE) American Association of Clinical Endocrinologists, (ADA) American Diabetes Association, (BG) blood glucose, (CF) correction factor [insulin sensitivity factor], (CIR) carbohydrate-to-insulin ratio, (CVS) cardiovascular surgery, (DM) diabetes mellitus, (ICU) intensive care unit, (IHI) Institute for Healthcare Improvement, (IV) intravenous, (POD) postoperative day, (RAI) rapid-acting insulin, (SC) subcutaneous insulin, (TDD) total daily dose of insulin.
Acknowledgements
The authors thank the diabetes resources personnel, supervising nurses in the CV surgery, ICU, and general surgical floor for help in planning the protocol, and all of the staff in each of those groups for their enthusiastic help in applying the protocol so successfully. The authors also thank Jennie Mattia, R.N., of the Fuqua Heart Center at Piedmont Hospital.
References
- Van den Berghe G, Wou ters P, Weekers F, Verwaest C, Bruynincks F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345(19):1359-67.
- Furnary AP, Gao G, Grun.kemeier GL, Wu Y, Zerr KJ, Bookin SO, Floten HS, Starr A. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003;125(5):1007-21.
- Krinsley JS. Effect of intensive glucose management on the mortality of critically ill adult patients. Mayo Clin Proc. 2004;79(8):992-1000.
- Krinsley JS, Grover A. Severe hypoglycemia in critically ill patients: risk factors and outcomes. Crit Care Med. 2007;35(10):2262-7.
- American College of Endocrinology and American Diabetes Association consensus statement on in-patient diabetes and glycemic control. Endocr Pract. 2006;12(14):458-68 and Diabetes Care. 2006;29(8):1955-62.
- Institute for Healthcare Improvement . Available from: www.IHI. orglIHIITopics/PatientSafetyl SurgicalSiteinfections/Changes/SSJ+ Maintain+Glucose+Control.htm.
- Richardson PR, Steed RD, Davidson PC. Immediate correction of hypoglycemia without rebound using variable dosing of IV glucose. Diabetes.1999;48(Suppl l):A120.
- Davidson PC, Steed RD, Bode BW. Glucommander, a computer directed intravenous insulin system, shown to be safe, simple, and effective in 120,618 h of operation. Diabetes Care. 2005;28(10):2418- 23.
- Davidson PC, Hebblewhite HR, Bode BW Steed RD, Welch NS, Greenlee MC, Richardson PL, Johnson J. Statistically-base CSII parameters: correction factor, CF(1700 rule), carbohydrate-to-insulin ratio, CIR (2.8 rule), and basal-to-total ratio. Diabetes Technol Ther. 2003;5(5):A237.