![]()
Presentation
American Diabetes Association Scientific Sessions
Date
June 2016
Authors
Joseph Aloi,1 Raymie McFarland,2 Robby Booth,2 Amy Henderson2
BACKGROUND
Dysglycemia has been shown to have a negative impact on patient outcomes including readmissions. Many acute illnesses can result in stress hyperglycemia, even for patients without diabetes. Sepsis is a prime example of stress-related dysglycemia due to an acute illness. The aim of this retrospective study is to determine if patients experiencing sepsis-related dysglycemia treated with intravenous (IV) insulin Glucommander, a computerized insulin dosing algorithm, have different outcomes compared to patients treated with standard insulin protocols and order sets.
METHODS
Patients with a diagnosis of sepsis (n=340) were treated with Glucommander (GM) IV or traditional IV insulin protocols (NonGM) for dysglycemia. Patients studied included type 1 & 2 Diabetes Mellitus and patients with hyperglycemia without a diagnosis of diabetes. All patients were evaluated for differences in:
- % of blood glucose (BG) in target glucose range of 70-180 mg/dl
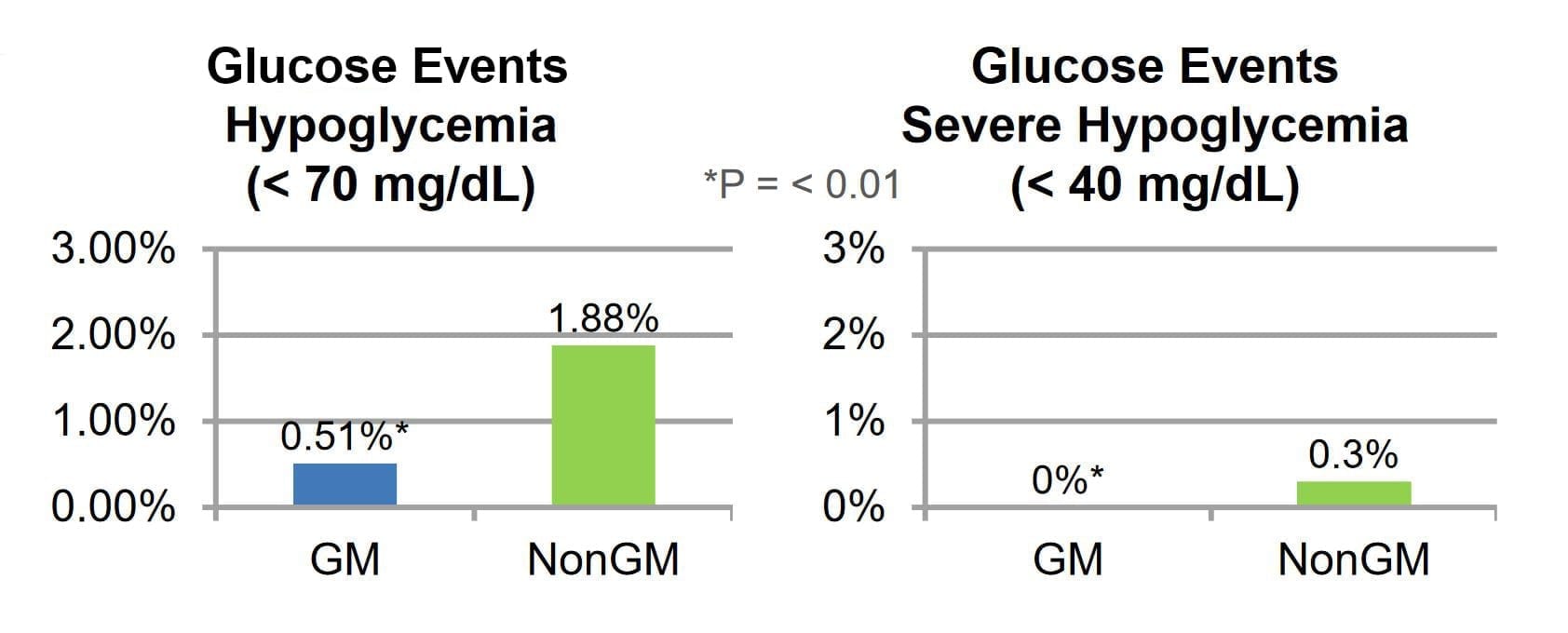
- % of Mild, Moderate and Severe Hypoglycemia (BG <40, <50, <70 mg/dL, respectively)
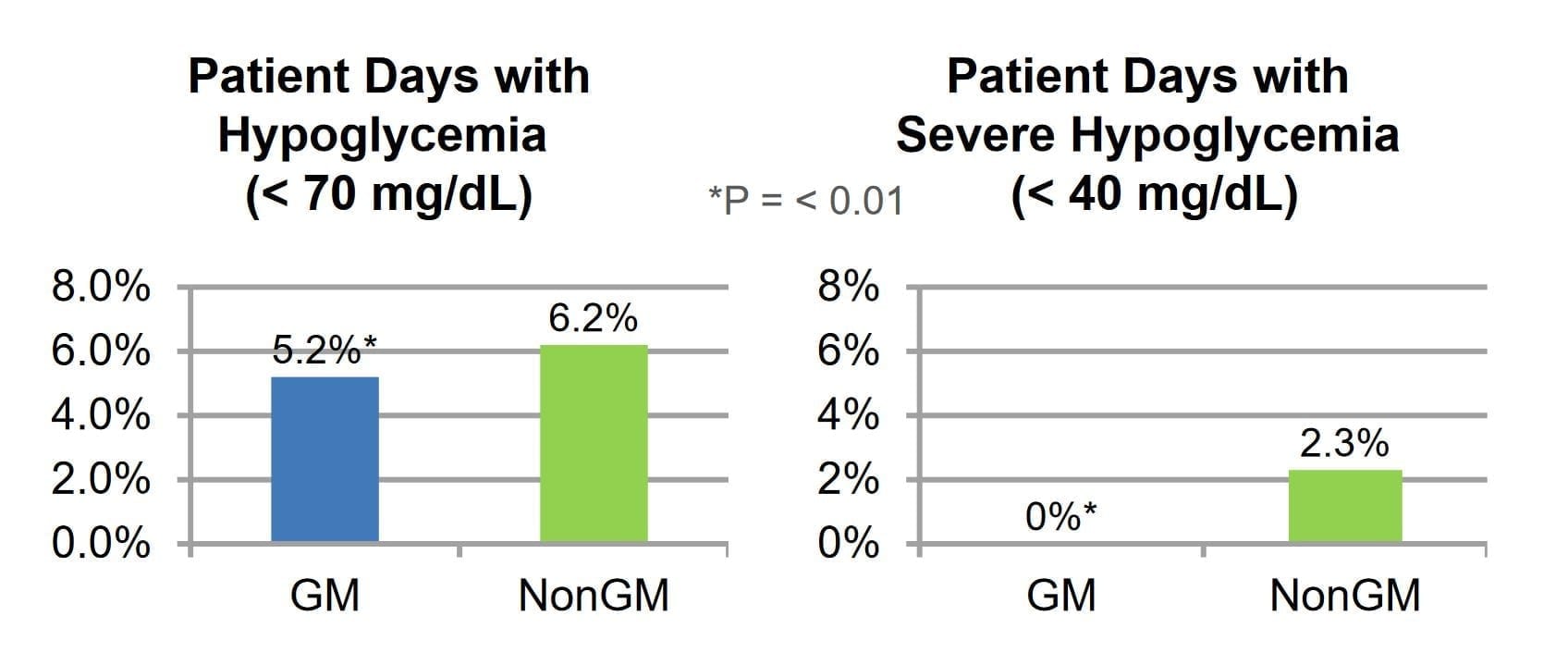
- Patient Days with Mild, Moderate and Severe Hypoglycemia (BG <40, <50, <70 mg/dL, respectively)
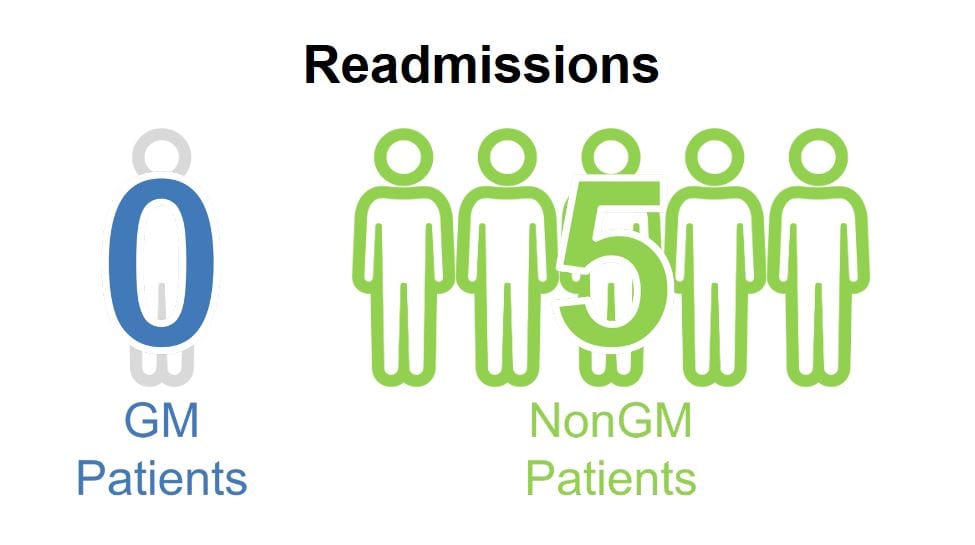
- 30-day hospital readmissions
RESULTS
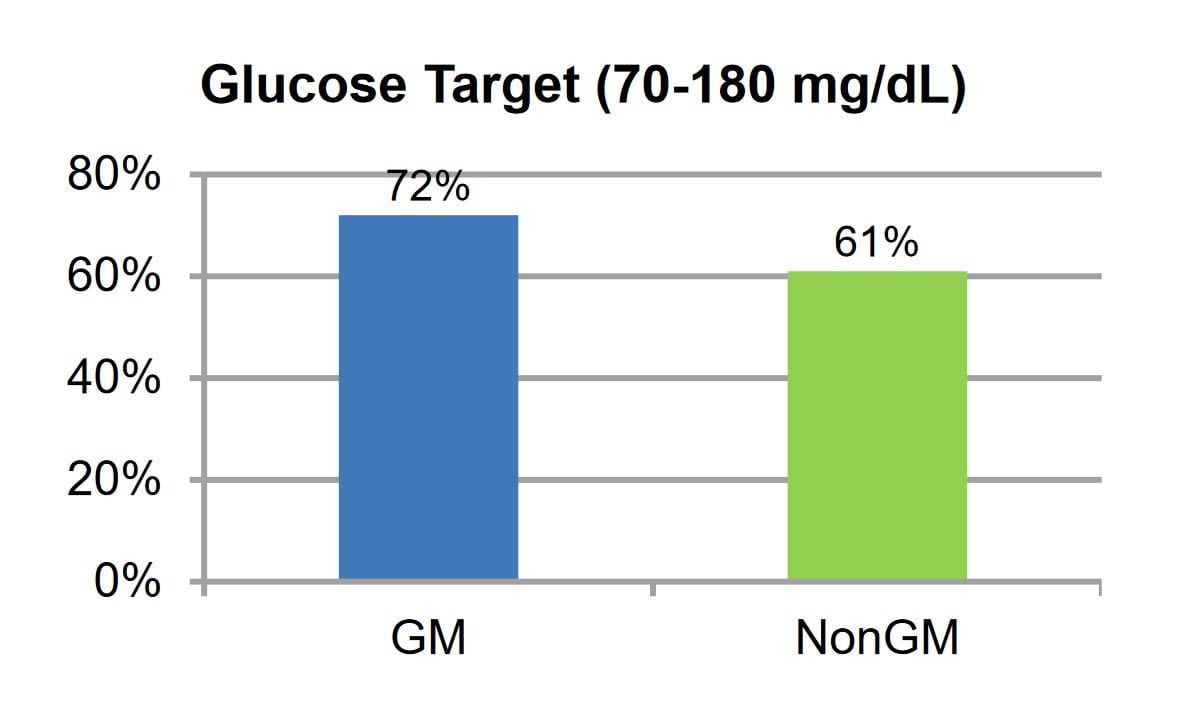
Patients treated with IV insulin utilizing GM had a higher percent in target range with 72% vs. 61%, a lower hypoglycemia rates; BG less than 70 mg/dL at 0.51% vs. 1.88% and a lower severe hypoglycemia % of BG with GM at 0.0% vs. 0.3%. Days with hypoglycemia <70 mg/dL was lower with GM at 5.2% vs. 6.2% and days with severe hypoglycemia <40 mg/dL was also lower with 0.0% for GM and 2.3% for NonGM. Readmissions were very low in both groups with GM having 0 patients and NonGM only having 5.
CONCLUSION
Glucommander use resulted in a significantly higher percentage of BG values in the prescribed glucose target range and significantly less glucose values and patient days with overall and severe hypoglycemia compared to traditional IV insulin protocols. Larger prospective studies are needed to analyze the impact on LOS, readmissions and mortality for patients with sepsis-related dysglycemia treated using standard IV insulin protocols or usual care compared to computerized insulin algorithms.
Affiliations
- Wake Forest School of Medicine, Winston Salem, North Carolina.
- Glytec, Waltham, Massachusetts.