![]()
Presentation
American Diabetes Association Scientific Sessions
Date
June 2015
Authors
Cora Espina, Lenise Taylor, Rafic Farah, Eunipi Cho, Joshua Epworth, Lori Jarrett, Ted Gooley, Paul O’Donnell, Irl Hirsch, Merav Bar
Background
- Allogeneic hematopoietic cell transplantation (HCT) is the only potential curative treatment for patients with high-risk hematological malignancies.
- HCT is associated with up to 30% Non-Relapse Mortality (NRM) over 200 days.
- Hyperglycemia, hypoglycemia, and increased glucose variability are associated with increased NRM, therefore, improving glycemic control may improve transplant outcome.
Aim
To evaluate the utility of a e-Glycemic Management System (eGMS) to improve glucose control in hospitalized HCT patients.
Patient Population
19 Allogeneic HCT Patients
| Demographic | n (%) or Median |
|---|---|
| Male | 14 (74%) |
| BMI kg/m2 | 29.2 (range 18.8-40.9) |
| Age (y) | 52 (range 22-73) |
| History of T2DM | 3 (16%) |
| Clinical Characteristics | n (%) or Median |
|---|---|
| On Systemic Steroids | 18 (95%) |
| On TPN | 8 (42%) |
| Blood Glucose (BG) Prior to Start (mg/dL) | 225 (range 158, 405) |
| Daily Prednisone Dose at Enrollment (mg) | 130 (0, 200) |
Results
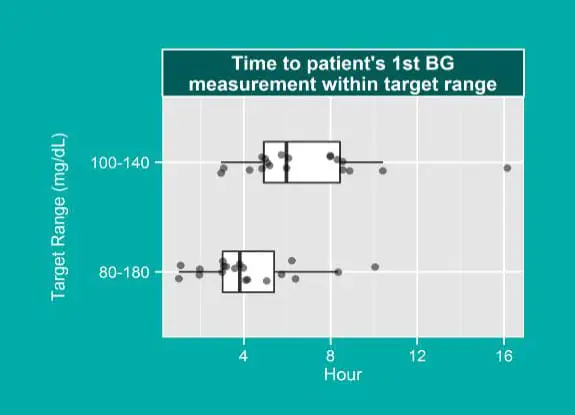
- All patients reached target BG (100-140).
- Median time to target was 6 hours.
- Median time to hospital standard (80-180) target was 4 hours.
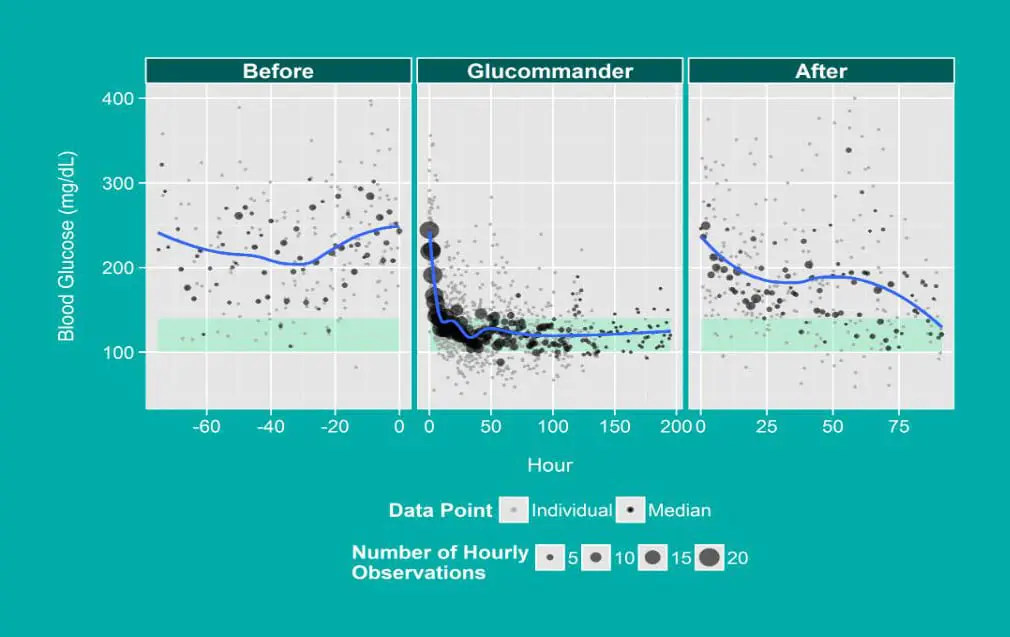
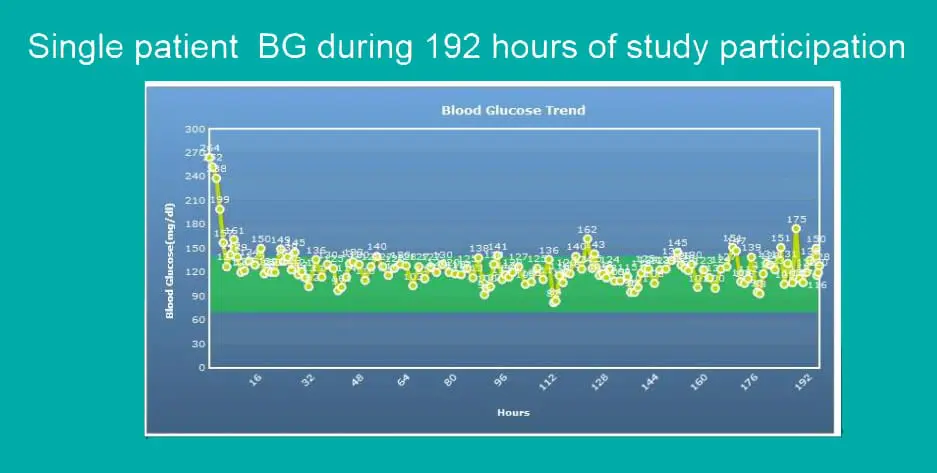
- Target BG levels were attained 82% of the time while on eGMS, whereas wide glycemic variability occurred without its use.
- Tight glucose control was achieved:
-
- with only 6 episodes of BG <70 mg/dL (0.5%);
- without severe hypoglycemia (BG <40 mg/dL).
- 74% (N=14) patients remained on eGMS for >24 hours.
- Patients were removed from protocol due to:
-
- transition from IV insulin to SC insulin (n = 4);
- discharge from hospital (n = 3);
- transition from IV insulin to insulin in TPN (n = 6);
- patient request due to frequent BG checks (n = 3).
Discussion
Despite high doses of steroids, TPN and unpredictable oral intake, tight BG control using an eGMS was achieved.
Study limitations did not allow for the standard integration of eGMS with the Electronic Medical Record (EMR).
Nursing Perspective:
- Duplicate entry of glucose and insulin doses in EMR and eGMS.
- “Timer” on eGMS gave opinion of more frequent BG checks.
- Unfamiliarity with aggressive glucose management protocol increased concern of potential for hypoglycemia.
- Anecdotally some felt blood glucose was better controlled and preferred to care for patients on eGMS.
Conclusions
- Achieving good BG control without frequent hypoglycemia in this challenging population is possible with eGMS.
- Future studies, which may include merging eGMS with Continuous Glucose Monitoring (CGM) system, are needed to eventually develop outcome studies.
Acknowledgments
Cora Espina and Lenise Taylor contributed equally to the study.
Kevin Coleman, Juan Pinelli, Shelly Mentzer recruited subjects.
Glytec, LLC provided the Glucommander software.
Affiliations
University of Washington Medical Center/Fred Hutchinson Cancer Research Center, Seattle, Washington.