![]()
Presentation
American Association of Clinical Endocrinologists Scientific & Clinical Congress
Date
May 2015
Authors
Melanie Mabrey,1,2 Jagdeesh Ullal,3 Raymie McFarland,1 Robby Booth,1 Amy Henderson,1 Joseph Aloi4
Objective
Acute myocardial infarction (AMI) patients presenting with hyperglycemia on admission have a higher mortality risk regardless of prior history of diabetes. A more specific marker for this increased risk is persistent and unresolved hyperglycemia. Proper screening for, and resolution of hyperglycemia in patients with AMI has been shown to have an impact on mortality. Many hospitals are challenged with implementing a comprehensive and standardized approach for identification of hyperglycemia and subsequent glycemic management. This study attempted to determine if Glucommander, a computerized intravenous and subcutaneous insulin-dosing algorithm can identify patients in need of intervention and be an effective method of improving glycemic management in patients with AMI. Most importantly, if it is possible to improve hyperglycemia without a subsequent increase in hypoglycemia.
Methods
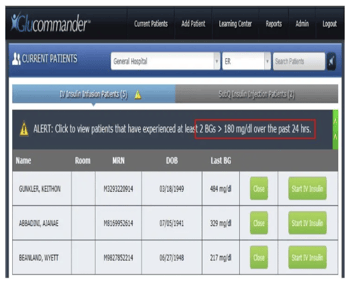
222 patients identified with GlucoSurveillance as having two blood glucoses (BG) >180 mg/dL within 24-hour period were randomized to an intravenous (IV) insulin dosing regimen, and then transitioned to subcutaneous insulin therapy.
- Arm 1 = Glucommander IV and SubQ
- Arm 2 = Standard paper order sets.
- Glucose target = 120-180 mg/dL.
- Measured outcomes:
- General demographics.
- Average glucose reduction.
- Percent of glucose readings in target.
- Hypoglycemia: mild (<70 mg/dL) and severe (<40 mg/dL).
- Average glucose on day of discharge.
Results
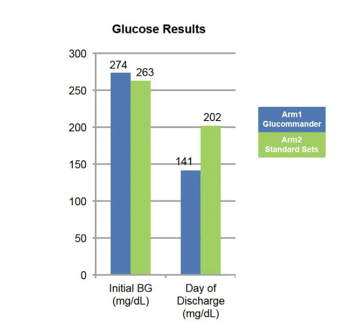
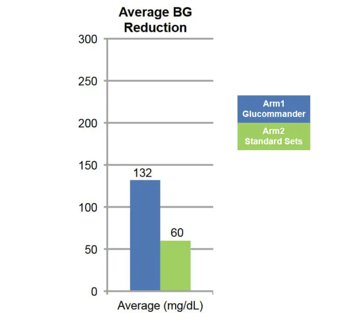
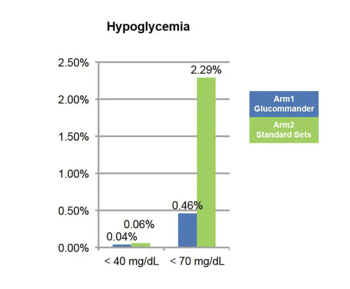
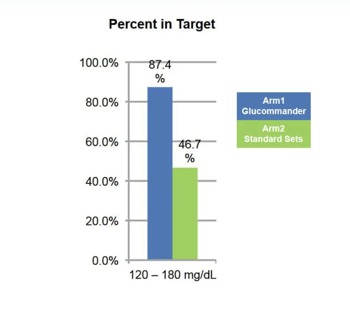
Arm 1 – 109 patients, average age of 64 years, A1c of 8.4 and an initial BG of 273.7 mg/dL. The average BG reduction was 132.3 mg/dL with 87.4% of glucose readings within target range. Hypoglycemia <70 mg/dL was 0.46% and <40 mg/dL was 0.04% and average glucose day of discharge was 141.4 mg/dL.
Arm 2 – 113 patients, average age of 66 years, an A1c of 8.8 and an initial BG of 262.8 mg/dL. The average BG reduction was 60.9 mg/dL with 46.7% of glucose readings within target range. Hypoglycemia <70 mg/dL was 2.29% and <40 mg/dL was 0.06% and average glucose day of discharge was 201.9 mg/dL.
| Arm 1 Glucommander |
Arm 2 Standard Sets |
|
|---|---|---|
| Patients w/AMI | 109 | 113 |
| Average Age | 64 | 66 |
| A1c | 8.4 | 8.8 |
| Initial BG | 274 | 263 |
Conclusion
Our results suggest using eGlycemic Management Solution (eGMS) with GlucoSurveillance to identify patients with hyperglycemia and AMI, then initiate and manage insulin with Glucommander in the hospital improves BG control. Patients achieve glucose target range at a higher percentage than standard paper order sets with less hypoglycemia. Additionally, patients were more likely to be discharged with blood glucoses in target. Further study is needed to assess implications for possible reduction in readmission and recurrent AMI as seen in DGAMI.
Affiliations
- Glytec, Waltham, Massachusetts.
- Duke University School of Nursing, Durham, North Carolina.
- Eastern Virginia Medical School, Norfolk, Virginia.
- Wake Forest Baptist Medical Center, Winston Salem, North Carolina.