![]()
Presentation
HMO Research Network Conference
Publication
Clinical Medicine & Research
Date
April 2014
AUTHORS
Deepa Ponnusamy, Veronica Piziak, Sonal Patel, Rhonda Urbanosky
BACKGROUND
Glucose management after cardiac surgery in our hospital was done using a locally developed paper insulin infusion protocol. Prolonged time to achieve and maintain target blood glucose was common and hypoglycemia was a significant problem. A computerized algorithm for insulin infusion was implemented and compared to the paper insulin infusion protocol. A barrier to effective implementation of this practice change was timed glucose measurements that consumed more nursing time. This was overcome by increasing nursing education and thereby efficiency. Hyperglycemia after meals and rapid glucose changes with glucose altering medications was addressed by adding extra glucose readings to allow the system to adjust the infusion rate.
METHODS
In order to assess the effectiveness of the new system, permission was received from the IRB to perform a retrospective chart review. Data for the paper protocol was obtained from 248 patient records during the time period of 7/1/11 to 12/30/11. Data for the computerized system was obtained from 181 patient records during the period of 8/1/12 to 5/2/13. Primary endpoints were time to achieve target glucose and hypoglycemia occurrence rates before and after intervention. The data was analyzed for time to achieve target glucose using a comparison of means and sample confidence levels for means of normal distributions with unknown variances.
RESULTS
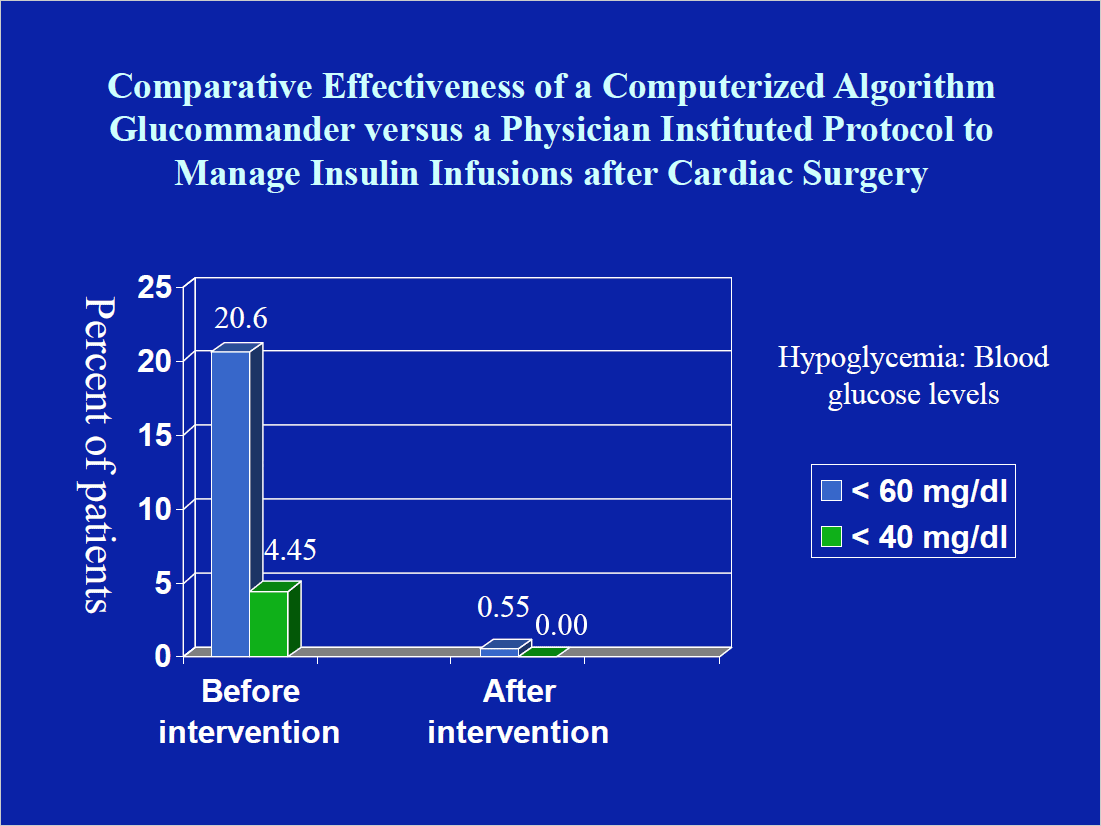
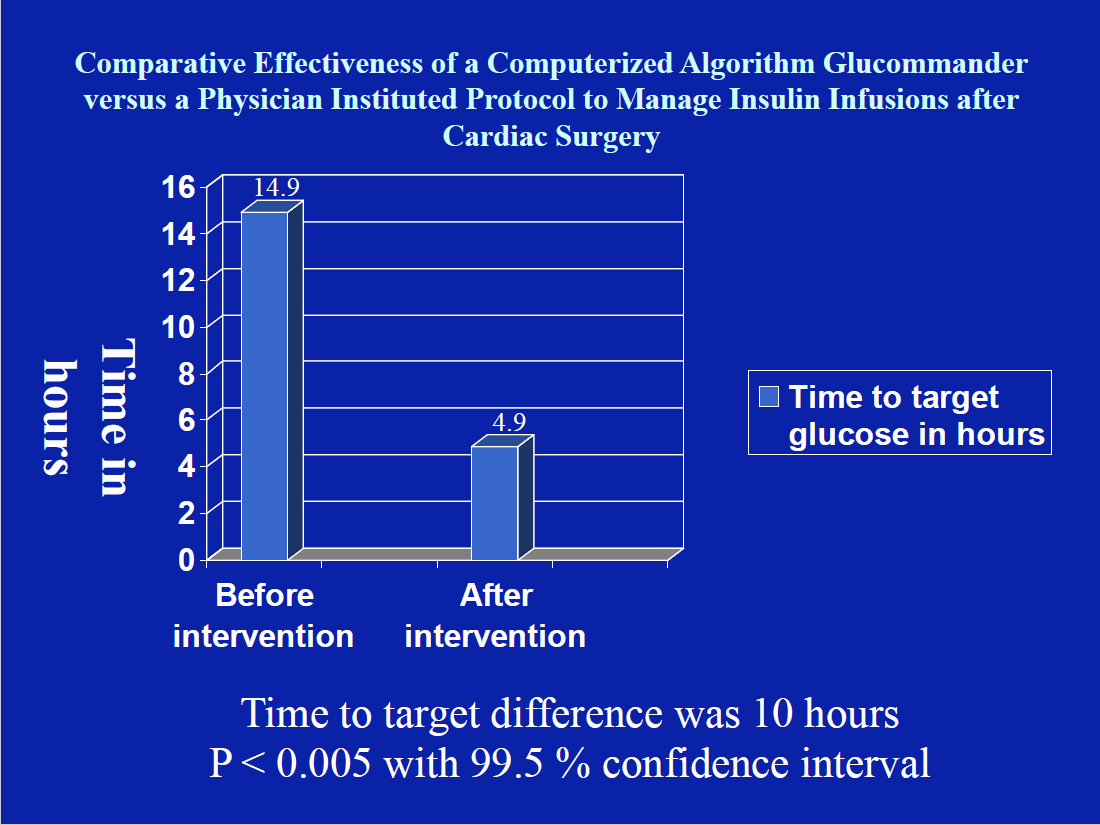
Mean time to achieve target blood glucose before the intervention was 14.9 hours, and after the intervention was only 4.9 hours. Difference in time to achieve target glucose was 10 hours (P <0.005 with 99.5% confidence level). Percent of patients with blood glucose <40 mg/dL was 4.45% (11 of 248) and blood glucose < 60 mg/dL was 20.6% (51 of 248) before the intervention. With the computerized insulin algorithm, percent of patients with blood glucose <40 mg/dL was 0.0% and <60 mg/dL was 0.55% (1 of 181).
CONCLUSIONS
The management of postoperative insulin infusions with a computerized algorithm results in significant improvement in patient care delivery with more efficient glucose control, little hypoglycemia, and an average saving of 10 hours of intensive care stay and nursing time. The health economic implications of this finding are being studied.